Two science historians discuss the historical association of disease, shame, and social stigma.
A public health announcement taken from a 1918 issue of Illustrated Current News is part of the Mütter Museum’s “Spit Spreads Death” exhibition. (Image: U.S. National Library of Medicine)
One of the early cases of COVID-19 spread within the United States happened at a glamorous birthday party in Westport, Connecticut. The event included dinner and dancing with guests that flew in for the occasion, including a man from Johannesburg, South Africa, who developed symptoms on the flight home. Yet the party host would not disclose the guest list to public health officials for contact tracing.
Shame and social stigma, says David Barnes, associate professor in the History and Sociology of Science Department, “is a huge issue in public health.” Ramah McKay, also of History and Sociology and Science, says people try to manage the information about who is infected because of shame. Researchers often describe stigmas as a problem of “spoiled identity, where your social identity becomes compromised. Or as a form of social death,” she says. “The stigma becomes a breaking of social ties.”
When negative health outcomes are tied to a situation where people are fearful of how that information will travel and how people will respond, secrecy ensues, McKay says. “In the public health sector, that prevents people from seeing how widespread COVID-19 is becoming, contributing to misinformation.” This was true with HIV as well, she says.
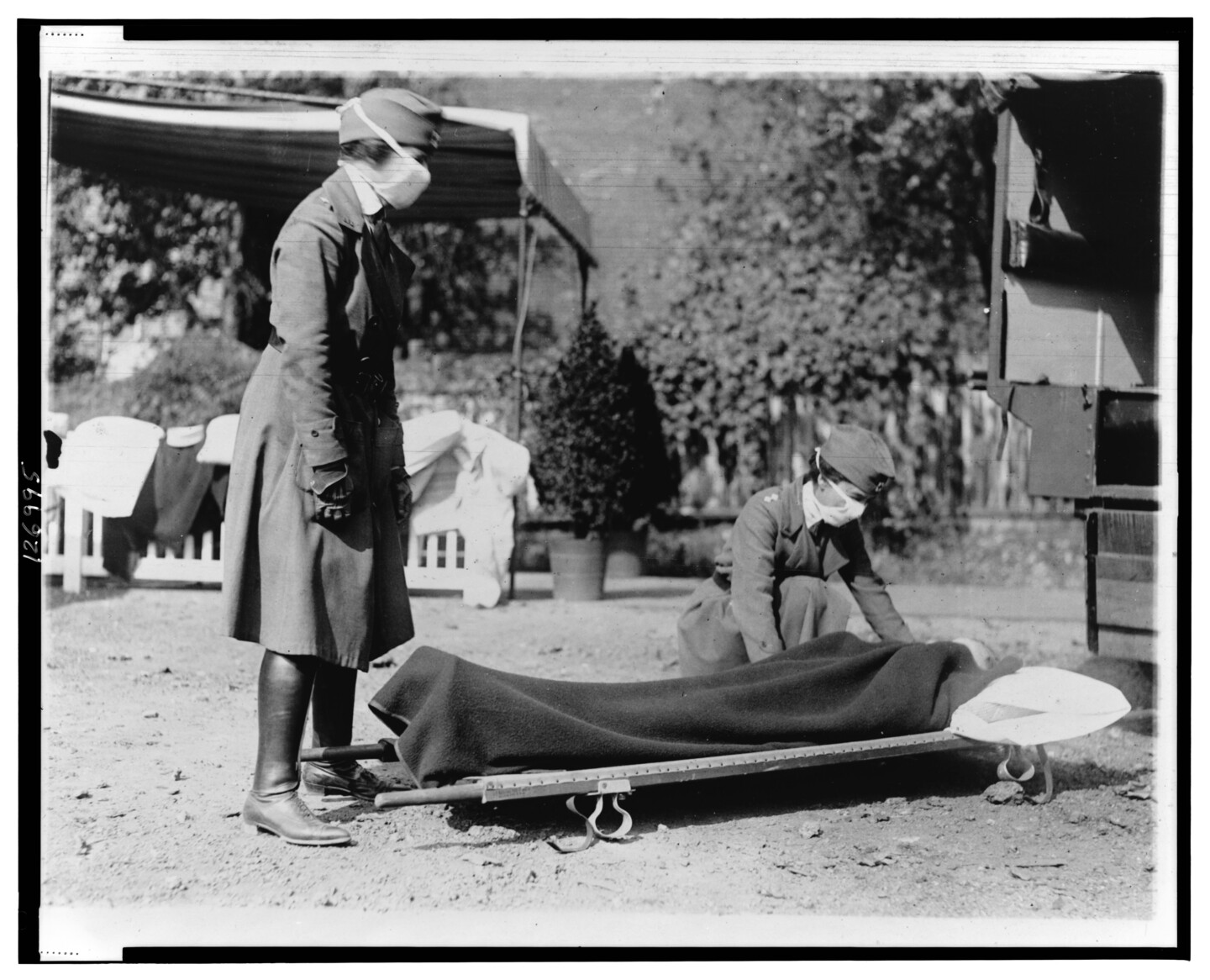
Demonstration at the Red Cross Emergency Ambulance Station in Washington, D.C., during the influenza pandemic of 1918. Part of the Mütter Museum’s “Spit Spreads Death” exhibition. (Image: National Photo Company Collection, Library of Congress Prints and Photographs Division)
“Stigma is rooted in fear,” she says. “When people fear there’s not a robust health response, that stigma goes up.” Anthropological accounts of Ebola virus disease, McKay says, have shown that once Ebola treatment units became more effective, fear surrounding the disease declined. McKay saw this in her research on HIV as well. As disease management was refined, “the messaging was, HIV is not something you need to hide, you can manage it.”
HIV/AIDS was “the most obvious example in my lifetime of a stigmatized disease,” Barnes says. “Everybody my age, everybody that lived through the peak years of that pandemic knows how widespread that stigma was,” which extended to the stigmatization of homosexuality as well, Barnes says.
Disease is stigmatized “because we’re afraid of getting sick and we’re afraid of dying,” Barnes says. “We take the things that we already fear and associate them with disease.
As COVID-19 moved from an outbreak to pandemic status, this fear manifested along racial lines. “The xenophobia in the early stages of this pandemic was acute,” Barnes says. “We saw the exact same anti-Chinese xenophobia with SARS in 2003.” The reports of racism and racial profiling towards Asians and Asian Americans was similar for West Africans when the Ebola virus peaked in 2014, McKay says.
The classic pattern of disease stigma is simply to shun people who show signs of illness, Barnes says. This can then extend to people belonging to marginalized groups, which can be “associated with spreading disease or illness or any kind of subversion,” Barnes says. “The essence of stigma and fear is that it is irrational. It feeds or comforts these primal ideas about ourselves and other people.”
Tuberculosis, however, was initially moralized as an elegant suffering, Barnes says. The afflicted were idealized in society and popular culture, Barnes says, citing John Keats, La Bohème, and Thérèse Martin as examples.
During this time, there was “a versatile and long-lasting cultural vision that associated tuberculosis with a heightened state of creativity, emotion, and spirituality, and that lent a tragic and redemptive quality to the disease,” Barnes writes.
Eventually, medical and philanthropic communities began to recast tuberculosis as a social disease that could be transmitted from person to person, often through unsavory behaviors.
Influenza precaution sign at Naval Aircraft Factory, Philadelphia Naval Shipyard, 1918. Part of the Mütter Museum’s “Spit Spreads Death” exhibition. (Image: U.S. Naval History and Heritage Command Photograph, Catalog # NH 41731-A, Archives Branch, Naval History and Heritage Command, Washington, D.C.)
These practices, already associated with the working classes and the peasantry, were attached to the new science of bacteriology that explained disease transmission, Barnes says.
As an example, he cites spitting, “which had gone from an accepted behavior part of everyday life almost like breathing and gradually over the course of a few centuries in civilized or bourgeois society, it came to be disgusting.” There were active campaigns against spitting, and it was prohibited in public, Barnes says, citing the “Spit Spreads Death” exhibition at the Mutter Museum that highlights a Philadelphia public health campaign during the 1918-19 influenza epidemic.
During a particularly virulent outbreak, shunning and stigma can extend to family relationships, Barnes says. “One of the most poignant description comes from Benjamin Rush writing about the yellow fever epidemics in the 1790s in Philadelphia,” Barnes says. “The greatest sorrow to Rush was seeing his city fall apart and to see neighbors forsaking neighbors and family members abandoning family members because they were so afraid of getting yellow fever and dying.
The Lazaretto, a historic Philadelphia quarantine hospital used to treat yellow fever, among other diseases. (Image: David Barnes, 2019)
“The most basic unit of society is your family,” Barnes says. “You don’t abandon them when they need you.” Rush characterized this abandonment, Barnes says, as “the ultimate horror of an epidemic. He paints this impressionistic portrait of a society in collapse.”
One of the new aspects of the COVID-19 pandemic is an emerging realization that recovered patients “may be a tremendous asset,” Barnes says. In addition, masks have become widespread. “At first, I thought I noticed a soft stigma surrounding that, and people would give those wearing masks a wide berth,” Barnes says. “But now that everyone’s wearing masks and everyone’s giving a wide berth to everyone, it’s mitigating that stigma.”
Nanoparticle blueprints reveal path to smarter medicines
New research involving Penn Engineering shows detailed variation in lipid nanoparticle size, shape, and internal structure, and finds that such factors correlate with how well they deliver therapeutic cargo to a particular destination.
A generous gift from alumni Glenn and Amanda Fuhrman brings the work of internationally acclaimed artist Jaume Plensa to the University of Pennsylvania. The latest addition to the Penn Art Collection expands Philadelphia's public art.
A massive chunk of ice, a new laser, and new information on sea-level rise
For nearly a decade, Leigh Stearns and collaborators aimed a laser scanner system at Greenland’s Helheim Glacier. Their long-running survey reveals that Helheim’s massive calving events don’t behave the way scientists once thought, reframing how ice loss contributes to sea-level rise.







{kind=link}
{kind=link}
{kind=link}