Decision-making and anxiety in the time of COVID-19
Penn experts discuss the psychology behind decision-making, how anxiety and stress impacts behavior, and share strategies for deciding how to safely reengage with society.
Many Americans remain concerned about contracting COVID-19 at the same time that stories of massive parties and unsocially-distanced concerts make headline news. As society grapples with what a “new normal” should look like, how do people decide which activities are safe, and why do some people’s choices look vastly different than others?
While more than half of Americans surveyed say that they are somewhat or very concerned about the novel coronavirus, viral stories of pandemic parties and unsocially-distanced concerts highlight the wide-ranging perspectives about the ongoing pandemic. As society grapples with what a “new normal” should look like, at the same time that the U.S. is still reeling from a summer surge in cases, how do people decide which activities are safe, and why do some people’s choices look vastly different than others?
Penn Today spoke with three experts in behavioral science to learn more about the cognitive basis of decision-making, how anxiety and stress impacts behavior, and what strategies people can use for making informed decisions on how to safely and comfortably reengage with society.
People make decisions by balancing risk with reward, and they don’t always do it rationally.
Psychologist Sudeep Bhatia and his Computational Behavioral Science Lab study the cognitive basis of human judgement and decision-making. One of his group’s areas of interest is risky decision-making, or how people make choices between options that have varying probabilities of payoff and risk.
While Bhatia says that economists and statisticians are interested in how these decisions can be made rationally, psychologists are interested in why the decisions that people make are not always rational. “We try to observe human behavior in terms of the operations of the mind to explain why people are being irrational, to figure out how a cognitive system that’s otherwise adapted to making good decisions still makes irrational decisions in certain cases,” he says.
To make a good decision, Bhatia says, one needs to know the probabilities for each outcome as well as some measure of the payoff. While it’s often straightforward to do the math and come up with a strategy that maximizes reward in the long-run, this isn’t what happens when, say, someone finds themselves deciding to bet all of their money on red five on a roulette table. Instead, people tend to overweigh small probabilities when assessing the probability of certain outcomes. “If there’s a 1% chance of something happening, be it winning a lottery or getting COVID, you are actually using a number than is bigger than it actually should be. This causes you to overestimate the probability of that low probability event,” he says.
But there’s an important caveat: “When you learn about probabilities by experiencing things in the world, you tend not to overestimate small probabilities but can also even sometimes underestimate small probabilities,” says Bhatia.
With COVID-19, learning from experience can lead to a polarization between how people perceive the riskiness of certain activities.
Bhatia says that while there are likely numerous and complex factors that influence how people perceive the pandemic, from partisanship to misinformation on social media, the psychology of decision-making, especially how experience informs risk perception, can help explain some of the discrepancies seen in people’s behaviors.
At the start of the pandemic, there was less personal experience with COVID-19 but lots of statistics about new cases and death rates, which then became over-weighted in people’s minds. “It means that the risk of COVID looms larger than it should,” he says. “But then, over time, people get experience, and when you get experience you start using your own behavior to inform what the risks are.”
As people gained more personal experience living with the pandemic, activities that have a small probability of risk can also perpetuate people’s varying perceptions of what activities are risky or not. For example, say a person engages in an activity with a 5% risk of contracting COVID-19. This means that the majority, 95% of people who participated, won’t get sick. “For small probability events, such as getting sick with a 5% chance, it takes quite a lot of experiences for you to actually get sick,” says Bhatia. “It means there’s a large number of people who have engaged in these activities who have not gotten sick and subsequently believe that the ‘gamble’ is good. The remaining people, however, have gotten sick, they might think this is a pretty bad deal, and that can lead to a polarization.”
Uncertainty and fear are common ingredients of both anxiety and COVID-19.
Thea Gallagher, clinic director of the Center for the Treatment and Study of Anxiety (CTSA) clinic at Penn’s Perelman School of Medicine, says that after the initial shock of shifting into “crisis mode,” many who might not have experienced symptoms of anxiety might now find themselves feeling more worried than before. “The core of anxiety is the intolerance of uncertainty and fear of the unknown, and I think nothing more exemplifies this time than those two phrases,” says Gallagher.
Along with an inability to plan for the future, legitimate fears about safety, health, and job security and abrupt changes to people’s support systems and coping strategies, it’s also a time when people are increasingly on edge, which can make anxiety even worse. “Everything is adding to people’s baseline level of stress and emotional reactivity, and the threshold for people to become emotionally upset is lower,” says CTSA Director Lily Brown. “Things that ordinarily might not affect them are much more impactful because everyone is at their wit’s end.”
Whether a person has clinical anxiety or is simply dealing with increased stress and worry because of the pandemic, the goal should be to find a healthy balance between trying to eliminate all risk versus ignoring the risks completely.
For patients with anxiety, Gallagher says, the tendency is often to try to eliminate all risks, which can lead some patients to be fearful of leaving their homes at all. The goal, she says, is helping patients find ways to reengage with society while making sure they are basing their decisions in facts over fear. “We challenge our patients to do something, but we also to lean into the fact that that this virus is contagious,” says Gallagher. “I use the example of driving: We get in our cars, but we don’t white knuckle it to the office. Instead, we live with that uncertainty, and we do our best.”
Seeing people at the extremes of anxiety, from being too afraid to do anything to engaging in very risky behaviors, is something that’s been observed in patients with PTSD, says Brown. “We’re seeing a lot of people bouncing back and forth, between excessive amount of concerns and then also somewhat unexpected risk-taking behavior,” she says, adding that this phenomenon could also explain why some people rush out to crowded places as soon as restrictions are lifted. “The goal here is to find that middle ground where you can be appropriately anxious where there’s legitimate threat but not so anxious that it’s making you not function. We think both of those are almost equally problematic.”
To help make productive and informed decisions, rely on guidelines from public health agencies, create a decision tree, and avoid getting stuck in “worry spirals.”
While it’s impossible to eliminate all risks of COVID without becoming completely isolated, Gallagher and Brown recommend that people experiencing any level of anxiety start figuring out what activities they are comfortable with based on guidance provided by public health organizations. For activities that people do decide to engage with, they also recommend creating a decision tree that includes considerations known to reduce coronavirus risk, such as being outside, wearing masks, and staying six feet apart from others.
They both caution against getting stuck in “worry spirals,” a common struggle for those with anxiety, where people try to make endless predictions about all of the hypothetical ways that something will happen and how they will deal with it. “Often, when people are stuck in this worry spiral, they think that they are problem solving and being productive, but they are actually engaging in strategies which not only don’t help them make effective decisions, it also worsens their anxiety in the long run,” says Brown.
To avoid getting stuck in a worry spiral, Gallagher recommends anyone who’s anxious to focus on controlling what they can in the moment without getting too far ahead. “I’m encouraging people to really hold loosely because outcomes are very unpredictable right now,” she says. “If there’s anything that this pandemic has taught us, it’s that we really need to be radically present. It’s really not worth trying to get out in front of it, people think that will bring them comfort and actually it just stresses them out.”
While the pandemic will certainly be a source of stress in the months to come, living with uncertainty and risk is not in of itself a new phenomenon. “It’s about using your best judgement, making a decision and committing to it, and leaning into the fact that there’s going to be risk everywhere,” says Gallagher. “We’ve lived with a lot of uncertainty and risk leading up to this point, and we can’t live our lives consumed by that fear and worry.”
Penn engineers and collaborators have developed a transparent, micro-engineered device that houses a living, vascularized model of human lung cancer—a “tumor on a chip”—and show that the diabetes drug vildagliptin helps more CAR T cells break through the tumor’s defenses and attack it effectively.
Tumor-on-a-chip offers insight into cancer-fighting cells in immunotherapy
Penn engineers and collaborators have built a living tumor on a chip to expose how cancers block immune attacks, and how one existing drug could make immunotherapy like CAR T more effective against solid tumors.
Professor of city and regional planning Erick Guerra recently published a book exploring the economic and societal impacts of American highways. He explains some of the pitfalls associated with an ever-expansive highway system, arguing that spending more on highways might not be the solution to the country’s transportation issues.
Penn urban planner Erick Guerra’s new book, “Overbuilt,” argues that additional spending on building more highways might not be the solution to the country’s transportation issues. In a Q&A, Guerra shares his insights.
Xin Sun prepares samples collected from the Eastern Tropical North Pacific aboard a research vessel. By adding stable isotope tracers to these vials, Sun and her team can track how different microbial groups convert nitrogen compounds into nitrous oxide, revealing how subtle shifts in oxygen and organic matter change the ocean’s chemistry.
Can tiny ocean organisms offer the key to better climate modeling?
In the shadowy layers of the Pacific, microbes decide how much nitrous oxide—a potent greenhouse gas—rises skyward. New research from Penn’s Xin Sun offers an improved understanding of microbial ecology and geochemistry—key to forecasting global emissions in response to natural and man-made climate change.
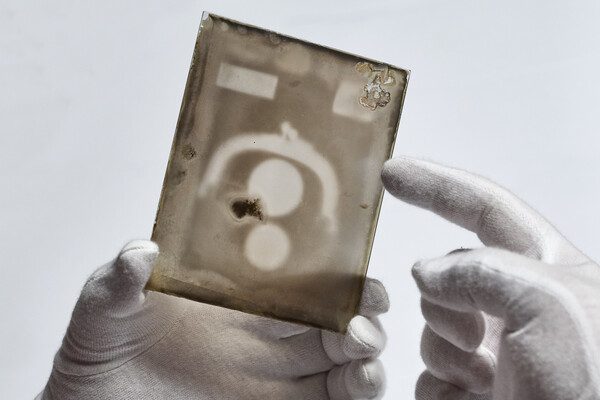
Two X-ray plates from Arthur Goodspeed, believed to have created the world’s first X-ray image, were donated by his family to Penn’s University Archives.