Around Penn, clinicians and researchers are focused on Ebola, working to ensure this disease—fearsomely lethal—can be vanquished.
In an experiment by the School of Veterinary Medicine’s Ronald Harty and Bruce Freedman, virus-like particles of Ebola (in green and yellow), which mimic the process by which the authentic Ebola virus spreads, exit a cell along filaments of actin (in red), a structural protein. Harty and Freedman are designing compounds to block this process, increasing the likelihood an infected individual could recover. (Image: Gordon Ruthel/School of Veterinary Medicine)
Ebola just isn’t going away. Following the major 2014 outbreak in West Africa, the deadly infection came back with a vengeance last year in the Democratic Republic of Congo, where it has claimed nearly 550 lives to date.
The impact has been felt closer to home as well.
Earlier this month, a patient at the Hospital of the University of Pennsylvania (HUP) was evaluated for Ebola. Having met the screening criteria for the disease—which include symptoms such as fever, head or muscle aches, or gastrointestinal symptoms, along with recent travel to West Africa—HUP took the cautious approach. Using the various protocols and precautions that they had trained to enact, hospital staff proceeded with evaluating the patient, who was later found to have another condition. This case, along with the ongoing Central African outbreak, underscore the need for continued vigilance when it comes to this disease.
At Penn, researchers and clinicians have been aiming their energy and expertise at Ebola, searching in the lab for drugs to treat it, in the clinic for strategies to safely contain it, and in the field to understand the social and societal factors that bear on it.
Though the disease has yet to have a significant impact in the U.S., it’s one that takes a global approach to tackle. At the Power of Penn in London event held last November, Penn President Amy Gutmann called out the disease as one example of why it is important for Penn to “transcend national boundaries and be global in our impact.”
An attack at the source
Researchers Ronald Harty and Bruce Freedman of the School of Veterinary Medicine have taken such a global approach for years. Long before the 2014 outbreak raised Americans’ consciousness about the disease, they’ve been collaborating with other scientists to find drugs to dispatch the infection.
Like many viruses, Ebola can mutate quickly, potentially evading the reach of some targeted therapies. The disease can also claim lives in short order. Those who don’t survive their infection can die within days. And while a vaccine for the virus exists, it’s not widely distributed. For these reasons, Harty and Freedman and colleagues have aimed their scientific investigations at developing an inhibitor compound that interferes with the interaction between the virus and the host it’s attempting to overwhelm.
A lasting collaboration between Penn Vet’s Freedman (seated) and Harty is giving rise to promising compounds for targeting Ebola. The pair’s company, Intervir, is now working to refine inhibitor molecules they hope will prove effective at quelling Ebola infections in animal models—and one day, humans. (Photo: John Donges/School of Veterinary Medicine)
For a virus such as Ebola to spread, it hijacks a host cell’s machinery, lacking its own equipment to carry out tasks critical to its ability to reproduce and spread. Blocking the virus’s ability to interact with host proteins is a strategy to limit infection. For Harty and Freedman, a specific target has been blocking budding, a process by which the virus slips out of a host cell after replicating itself inside.
“The idea behind the host approach is that, not only should it work against quickly evolving strains of the virus, because these interacting domains are critical to the viruses’ life cycle,” says Freedman, “but also other viruses often use similar mechanisms to interact with the host. So, much like using a broad-spectrum antibiotic to treat a bacterial infection, by using a drug that targets the host-viral interaction you may be able to block a half dozen or more different pathogens that utilize those same mechanisms.”
At Penn Vet, researchers use a variety of laboratory tests that don’t involve the actual viruses to screen compounds that might block budding and slow down the spread of the virus. One assay involves the generation in cells of virus-like particles, or VLPs, which bud by a process that mimics that of authentic Ebola virus. The second examines the protein-protein interaction between the specific elements of viral and host proteins involved in budding. And the third uses a related but non-lethal virus, vesicular stomatitis virus, to test the effectiveness of the viral inhibitors the team is screening.
We’re following the science and we’re learning a lot along the way. If we wind up with a drug that can help people, that will be something we’ll take to our graves as a life’s accomplishment.
Bruce Freedman of the School of Veterinary Medicine
“If all three of those look good,” says Harty, “then we know we have a good candidate to test with authentic Ebola virus.”
For those more-involved experiments, the Penn Vet team partners with colleagues at the U.S. Army Medical Research Institute of Infectious Disease (USAMRIID), which has a Biosafety Level 4 laboratory.
Already, those tests have generated solid data, and now Harty and Freedman are working with colleagues within the Fox Chase Chemical Diversity Center to improve upon the viral inhibitors they’ve identified.
“We’re seeing good results with Ebola but also with related hemorrhagic fever viruses like Marburg and Lassa fever,” says Harty. “The next big step, and that’s what we’re working on now, is to try to tweak one of these inhibitors so we can use it in an animal model to see if it works there.”
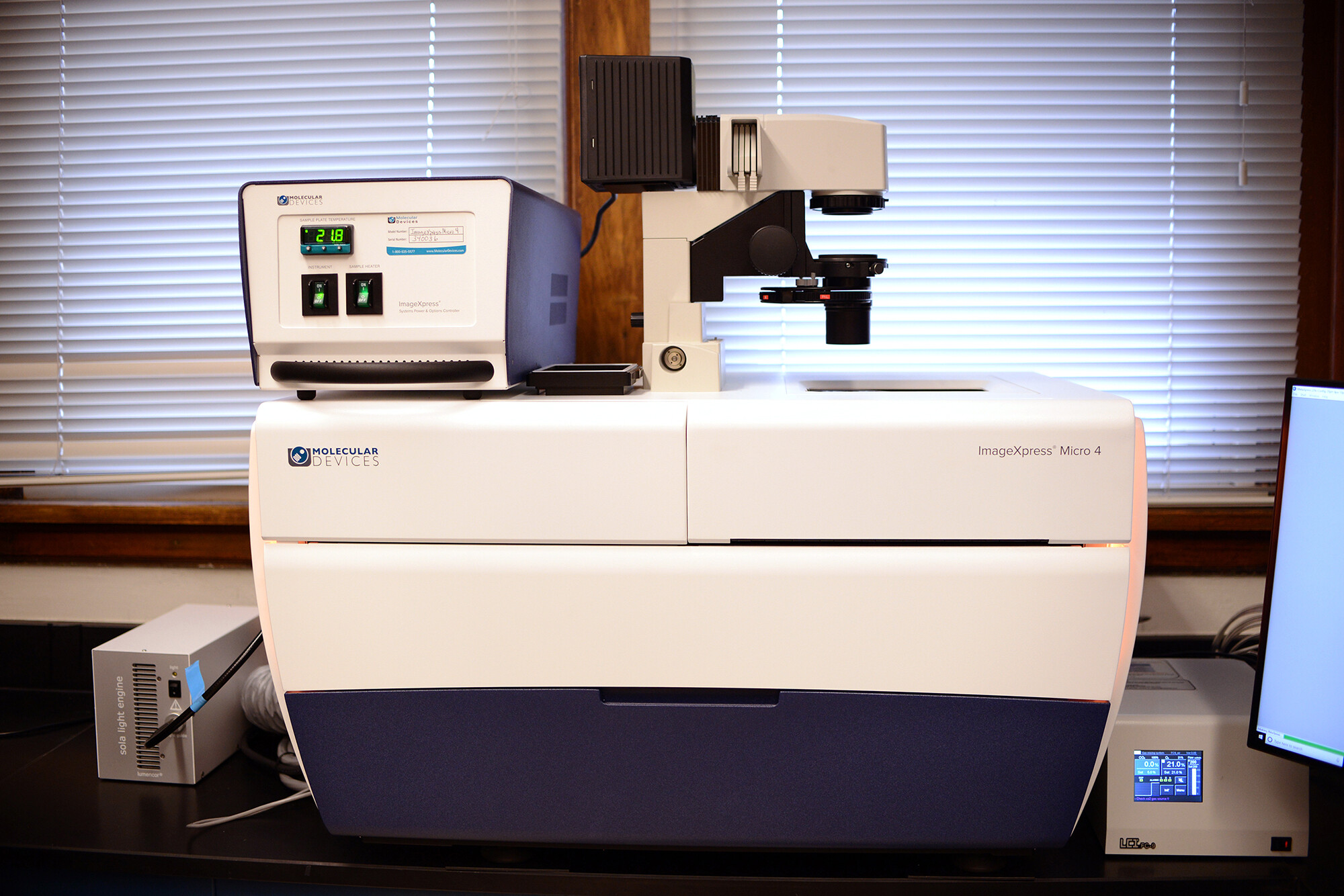
A new piece of equipment at Penn Vet, a high-content imaging system, will enable researchers to acquire images of whole organisms and cellular or intracellular events as they happen. The technology will be used to evaluate viral inhibitors. (Photo: John Donges/School of Veterinary Medicine)
Based on the promise of their findings to date, Harty and Freedman have launched a company, Intervir, to help refine and bring these inhibitors to market.
“The hope is that a therapeutic could be given to an individual who is positive for Ebola virus, to block the transmission or spread in that person or to dampen that spread and allow that person’s immune system more time to fight the virus,” says Harty. He likens such a drug to Tamiflu, which lessens the impact of the influenza in vulnerable individuals.
“We’re following the science,” adds Freedman, “and we’re learning a lot along the way. If we wind up with a drug that can help people, that will be something we’ll take to our graves as a life’s accomplishment.”
The Penn Vet researchers are not the only scientists at Penn attuned to the biology of Ebola in order to undermine it. Picking up on reports from the 2014 outbreak that Ebola could be sexually transmitted, the lab of Paul Bates in the Perelman School of Medicine examined how such transmission could occur. In a study published last year in the journal Proceedings of the National Academy of Sciences, Bates and colleagues described their discovery of how protein fragments found in semen, called amyloid fibrils, enhanced Ebola transmission and protected the virus from inhospitable hot and dry conditions.
Using a benign version of the Ebola virus in the lab, the Penn Medicine researchers found that pairing the virus with amyloids led to infection levels 20 times higher than those with the virus alone. As a next step, the team is beginning experiments to evaluate whether compounds that disrupt the amyloids can compromise Ebola’s ability to survive in semen and be passed on to others through sexual contact.
Gearing up
Such therapeutics as those envisioned by Bates, Freedman, and Harty could be of great use in a clinical setting, be it in Africa, or here in the U.S. Barring such effective therapies, however, clinics with the resources to do so must be prepared to offer as much support to Ebola patients as possible, all without compromising the safety of the caregivers themselves.
This was the challenge taken up by HUP in the summer of 2014, when, with the Ebola outbreak raging in West Africa, hospital leadership organized and executed an intensive bout of training and planning to prepare for treating Ebola patients.
“We felt a responsibility to the community to be prepared,” says Neil Fishman, chief medical officer for Penn Medicine. One encounter with a patient whom clinicians suspected might have Ebola but who claimed he hadn’t traveled outside the country recently, highlighted the need to do so. “I went to talk to him because I was curious,” says Fishman. “He said he hadn’t wanted to admit he had traveled to Africa because he was afraid that we wouldn’t care for him if he had Ebola.”
To assuage the fears of patients like this man, who wound up having malaria, Fishman worked with Cindy Morgan of Penn Medicine Academy and other health system leaders to rally a hospital-wide team, engaging everyone from environmental services to materials management to facilities in addition to doctors, nurses, and other caregivers. “These people volunteered to train and give up time on their evenings and weekends for this,” he recalls.
Fishman likes to say they built a hospital and trained an army in six weeks, and it’s not far from the truth.
“To give you an idea of how fast things went,” he says, “On a Friday we were discussing a concern about how to evaluate patients outside the emergency department without exposing other patients. The head of the department said it would be really nice if we had a room outside the ED where we could evaluate these patients. We came in Monday and it was built.”
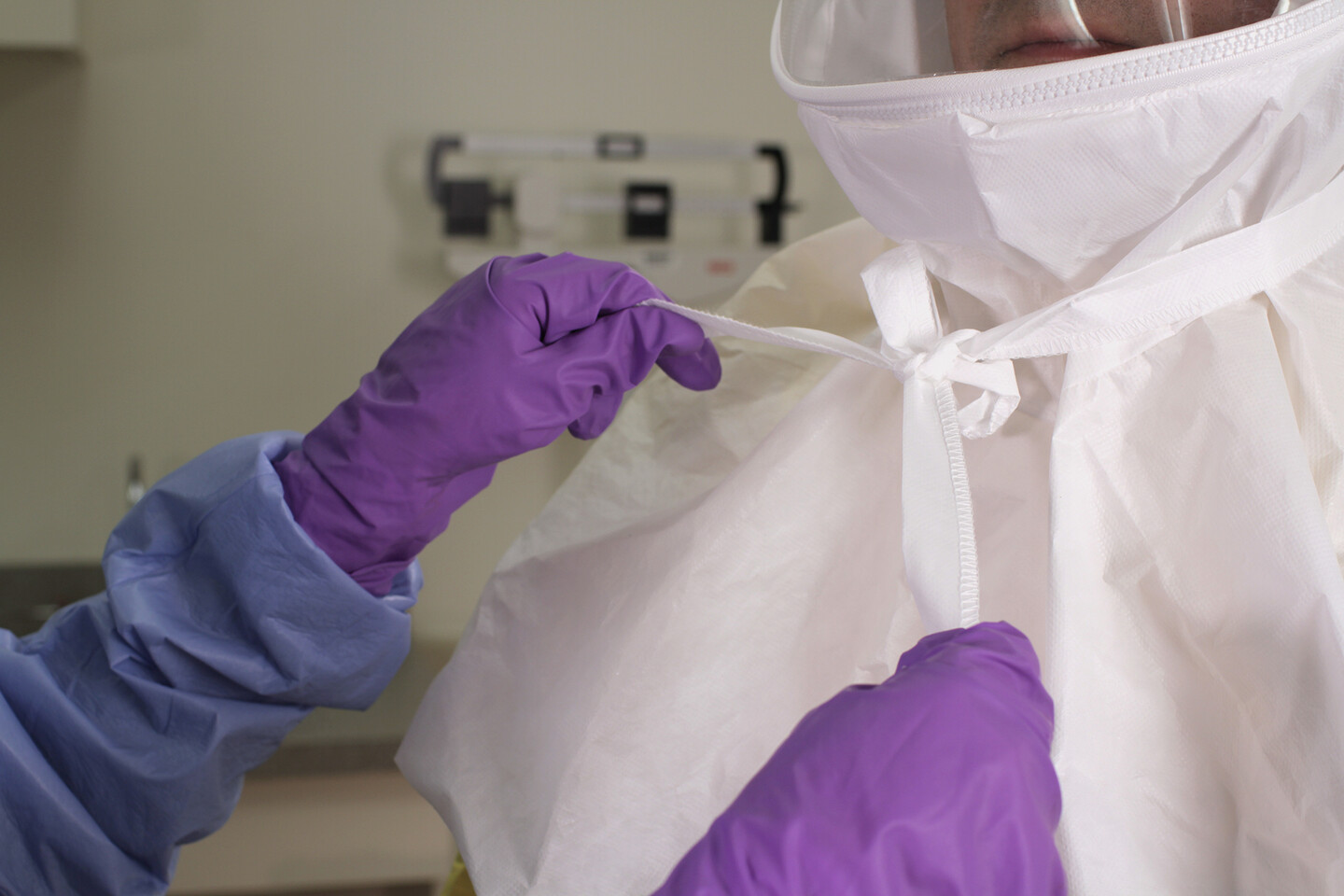
With a contagious disease such as Ebola, personal protective equipment plays a key role in providing safe care for patients. Staff at the Hospital of the University of Pennsylvania have received intensive training in providing this care, from properly donning and doffing equipment, to how to clean patients’ rooms. (Photo courtesy: Perelman School of Medicine)
In addition to constructing a new isolation unit, the team developed a litany of protocols to ensure patient and staff safety. They simulated placing IV lines, delivering babies, cleaning patients’ rooms, and transferring patients across the city.
In that period of heightened concern about Ebola, HUP evaluated several patients for the virus, all of whom ended up having malaria instead. HUP leadership also trained staff at other hospitals in the Penn Medicine system.
In the years since, to keep the team’s skills fresh, hospital workers have performed occasional drills, either table-top simulations or more hands-on trainings, donning and doffing personal protective equipment. They’re also keeping a close eye on the outbreak in the Congo, and continuing their protocol for screening potentially affected patients, as they did a few weeks ago.
But Fishman is aware that the next big infectious threat may not be Ebola. “It could be something else we’ve never seen before—like the SARS a few years ago, or the emerging Middle Eastern Respiratory Syndrome, or a totally new disease” he says. “In any case, we need to be prepared.”
What they did for Ebola in 2014 could provide a template for responding to future threats.
“It will inform our approach as we move forward,” Fishman says.
Remembering the caregivers
Unfortunately the resources accessible at Penn’s hospitals are not universally available. Health care workers in the heart of the Ebola outbreak in West Africa in 2014, and in Central Africa currently, often are not as well-outfitted to safely and effectively treat patients with the highly infectious disease.
As a trained nurse and a bioethicist, Connie Ulrich of the School of Nursing spent a lot of time considering the circumstances facing doctors and nurses in Africa during the 2014 outbreak. Penning an opinion piece in the British Medical Journal that fall, Ulrich began, “No one is talking about what must be profound moral distress among local African health care workers.”
A nurse and bioethicist, Connie Ulrich has written of the “moral distress” faced by health care providers who worked in the 2014 Ebola outbreak. “I really have not seen a situation that rivals Ebola in terms of the risk to health care workers.”
While nurses face stressful situations on a daily basis in the course of work, and encounter real risks to their health, be it from a sneezing patient or a needlestick, Ulrich contends that Ebola was different because the risks were so extreme.
“I worked as an OR nurse. I was exposed to the risk of needlesticks, blood and body fluids,” says Ulrich. “But I really have not seen a situation that rivals Ebola in terms of the risk to health care workers. Nurses and other health care workers who were on the front lines were dying in western Africa. And to some degree, this created a heightened anxiety and stress in the U.S. Knowing we live in a global society, nurses here were aware that any patient could walk into an exam room with flu-like symptoms and turn out to have Ebola.”
In under-resourced settings, Ulrich explains, health care workers can find themselves facing daunting ethical questions: Are they obligated to treat a patient if it puts themselves in grave danger of acquiring a life-threatening illness? Should they perform CPR on an Ebola patient if that increases those risks? What if the raw number of patients at a given clinic is too great to serve effectively? Should they pursue this work even if it means that their family will face social stigmas?
“We’re still thinking through many of these questions,” Ulrich says. “But for me, a lesson learned is that communication is absolutely key. We need to make sure that we’re communicating in a way that is transparent and effective about how health care workers should handle certain circumstances, what their obligations are to their patients, and what their institutions’ obligations are to them.”
These are issues that Ramah McKay, too, has considered, albeit through her own lens as a trained anthropologist. Though not focused on Ebola specifically, McKay has studied how health care systems in Africa and elsewhere have responded to infectious disease threats.
As McKay wrote about in her 2018 book, “Medicine in the Meantime: The Work of Care in Mozambique,” such unevenness is a feature of global aid for health care in developing nations, which often comes earmarked global aid for health care in developing nations often comes earmarked for one disease, such as malaria or HIV. One positive outcome of the recent Ebola outbreaks, McKay notes, is underscoring the limits of this approach to health care funding.
“There has been renewed attention to health system strengthening, or the idea that funding or international aid for health care should always be applied with an eye toward how will this create a robust health system, in addition to addressing the particular goal that we’re hoping to address,” she says. “If resources get concentrated in one area or focused on one disease, that produces weaknesses in other areas of the health system.”
As Ulrich has also noted, McKay says the recent outbreaks “bring to light the risks that health workers face when they’re working in an under-resourced environment.” While physicians and nurses with U.S. passports were in some cases flown to world-class clinics to be treated for Ebola if they became infected, many African health care workers died of their illnesses contracted on the job.
A possible outgrowth of these risks and ill-prepared health care settings is a mistrust by patients of the very workers and clinics who are doing their best to treat them. But McKay emphasizes that this mistrust “may be rooted not in ignorance but in experience.” People may have received poor care in the past, or been the subjects of research but not benefitted from that work.
“I think this is a problem but also an opportunity,” McKay says. “We can think about how to design interventions in an ethical and equitable way so that interventions now also produce better health in the future.”
Such forward-thinking is characteristic of Penn faculty’s approach to the threats of Ebola, not only considering the problems at hand today, but looking broader to generate knowledge that may help society when, and not if, the next threat arrives.
Ronald Harty is a professor of pathobiology and microbiology in the School of Veterinary Medicine.
Bruce Freedman is an associate professor and director of the Imaging Core Facility in the School of Veterinary Medicine.
Neil Fishman is chief medical officer, chief patient safety officer, and an associate professor of medicine in the Perelman School of Medicine.
Paul Bates is a professor of microbiology in the Perelman School of Medicine.
Connie Ulrich is the Lillian S. Brunner Chair in Medical and Surgical Nursing and professor of nursing in the School of Nursing and a professor of bioethics in the Perelman School of Medicine.
Homepage photo: Ebola virus particles, in red, affix themselves to a larger cell. Studies to identify therapies to treat or prevent the transmission of Ebola are ongoing on Penn. New findings suggest that the virus can unexpectedly persist—for years, in some cases—in the bodies of those who have been infected. (Credit: National Institute of Allergy and Infectious Disease/National Institutes of Health)
Materials in the Annenberg School for Communication Library Archives include thousands of TV scripts, the first issue of TV Guide, and interviews about the early days of HBO—which help to chronicle TV’s 100-year story.
Centering joy in AI development and implementation
PIK Professor Desmond Upton Patton—of Annenberg and SP2—and collaborators introduce a joy-informed framework designed to initiate conversations among engineers, designers, and researchers.
Winter Storm Fern brought icy and snowy conditions to the Northeast and other parts of the country over the weekend. Penn Today asks physicist Robert Carpick about the unique properties of ice, the science of curling, and how close we are to ‘nonslip’ ice.
Organizations like Penn’s Netter Center for Community Partnerships foster collaborations between Penn and public schools in the West Philadelphia community.
Penn receives national distinction for community engagement
The recognition by the American Council on Education and Carnegie Foundation for the Advancement of Teaching acknowledges Penn’s long-standing commitment to community-engaged scholarship and partnerships in West Philadelphia and beyond.








{kind=link}
{kind=link}
{kind=link}
{kind=link}