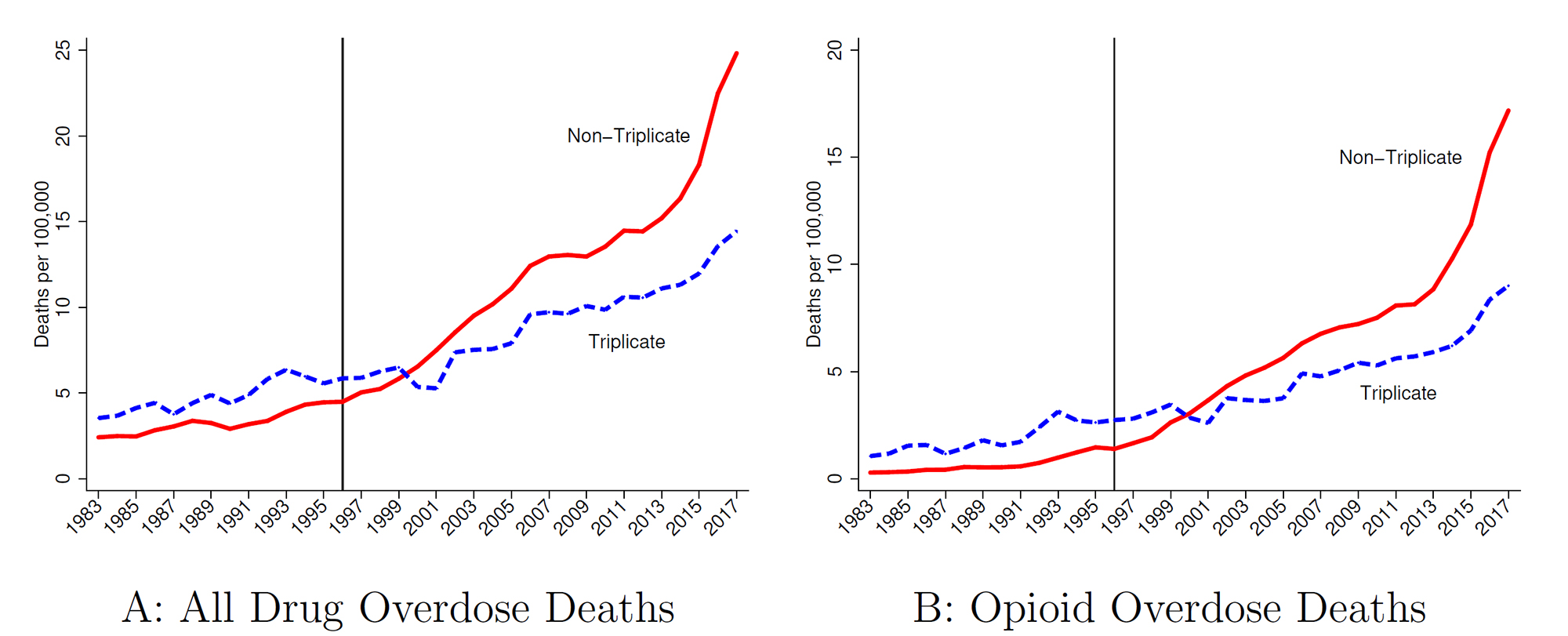
A state prescription drug policy first adopted in 1939, and last ended in 2004, appears to have influenced where Purdue Pharma chose to market its opioid drug OxyContin upon launch in 1996. The consequences of that decision reverberate to this day, according to a new study in The Quarterly Journal of Economics by LDI senior fellow Abby Alpert and colleagues, who estimate that states with the prescription policy had 11.3 fewer overdose deaths per 100,000 people in 2017.
Drug overdose deaths, by triplicate state status. Source: Alpert et al., NBER Working Paper 26500, 2019. (Image: Penn LDI)
The paper analyzes how public policy can influence and interact with commercial activities, leading to effects that could not be foreseen upon enactment of the policy. In the context of the opioid epidemic, these effects have had enduring impact on overdose deaths in the subsequent generation.
The policy was an early prescription drug monitoring program that required physicians to use a state-issued triplicate form when prescribing Schedule II controlled substances (which includes many opioids). The physician had to keep one copy on record. The patient took two copies to the pharmacy; the pharmacy kept one and sent the third copy to the state drug monitoring agency. The state agency maintained a database from these forms to monitor and investigate prescribing irregularities and diversion.
Triplicate programs had been effective in reducing prescribing of the drugs subject to the policy, due to physician concerns about tangible government oversight of their prescribing behavior and the hassle factor in handling and keeping records of the triplicate forms. “Triplicate states” are mentioned repeatedly in Purdue Pharma internal documents as having been important barriers to OxyContin prescribing, with lower expected returns from marketing spending. These documents suggest that less marketing was targeted to triplicate states, with one document recommending that “the product [OxyContin] should only be positioned to physicians in non-triplicate states.” Indeed, triplicate states had some of the lowest OxyContin adoption rates in the country.
By comparing trends in triplicate vs. non-triplicate states, Alpert and colleagues provide empirical evidence that the origins of the opioid epidemic lie in the marketing of OxyContin.
In Senegal, the ambitious Dakar Greenbelt project seeks to create an extensive network of ecological infrastructure in and around the city to sustainably address environmental concerns and enhance urban life. With support from David Gouverneur and Ellen Neises, Ph.D. candidate Rob Levinthal in the Weitzman School of Design led two courses that included a field trip to Dakar, that culminated in students presenting their visions for parts of the Greenbelt.
From a desert to an oasis: Penn engages in ambitious greening effort in the Sahel
Students from the Weitzman School of Design journeyed to Senegal to help with a massive ecological and infrastructural greening effort as part of their coursework. The Dakar Greenbelt aims to combat desertification and promote sustainable urban growth.
As part of an undergraduate course, Penn faculty and students curated an Arthur Ross Gallery exhibition of works from the Neumann family’s extensive collection of modern and contemporary art.
The University’s nexus for technology transfer supports researchers in their innovative efforts, from CAR T to mRNA advancements that have dramatically reshaped the world.