From the history of science to medical anthropology, governance, and economics, Penn experts look at the history of global health from different perspectives to see what the future may hold.
Researchers at Penn are focused on the interdependence of global health. “We’re all healthier if we’re all healthier,” says Ramah McKay (not pictured), a medical anthropologist in the School of Arts & Sciences. “Our health is always dependent on other people.”
Last October, professor Harsha Thirumurthy of the Perelman School of Medicine co-authored a paper stating, “a pathogen like influenza has the potential to travel around the world within hours and could kill tens of millions of people, disrupt economies, and destabilize national security.”
While this now seems prescient, the emergence rate of infectious diseases has been rising since the 1940s. A full 60% of these new diseases are zoonotic, meaning they can be transmitted from animals to people.
One Health: A connection between people, animals, and their environment
Contributing factors to this rise include human population growth and urbanization, habitat loss and fragmentation, overharvesting in trade and wildlife, globalization, and rapid, long-distance transport, says Julie Ellis, an ecologist at Penn’s School of Veterinary Medicine.
Ellis’ work focuses on the intersection of humans and wildlife. “The first place I usually like to start in these conversations is with the concept of One Health,” she says, citing the intersectional wellness approach. “Human health and animal health are tied together and are both bound to the natural ecosystem. Humans like to think that they’re somehow independent from natural ecosystems, but we’re not, and the COVID pandemic has demonstrated that.”
Harsha Thirumurthy, the Associate Director of the Center for Health Incentives and Behavorial Economics, Associate Professor of Medical Ethics and Healthy Policy, Perelman School of Medicine, and Senior Fellow at the Leonard Davis Institute of Health Economics.
The emergence of COVID-19 was likely born out of wet markets, “the perfect scenario for potential host switching of a virus,” Ellis says. “In some of the markets, you may have chickens, pigs, pangolins, a variety of animals both domestic and wild in close proximity.” This creates the opportunity for the spread of virus through bodily fluids and excrement, Ellis says.
COVID-19 originally existed in the unusually robust immune systems of horseshoe bats, studies suggest. Before coming to humans, the virus most likely had an intermediate host, with recent research suggesting the pangolin as a likely candidate, Ellis says. When humans and animals are in close quarters, there’s a higher probability that a virus will hop between animal species, and on to humans.
Humans also come into close contact with animals through deforestation, cutting down trees in order to replace them with farms or to sell the wood for income. “People tend to think of wildlife bringing these diseases to us, but in fact we’re bringing it upon ourselves in terms of our intrusion into their habitats,” Ellis says.
She references the 1998 emergence of the Nipah virus in Malaysia. As farmers intensified food production in forested areas, they cleared trees in order to build increasingly large piggeries. On the edges of pig sties, Ellis says, they planted fruit trees for additional income. Fruit bats, attracted to the trees providing their food source, would eat the fruit, later dropping pieces onto the ground where the pigs were kept. Ingestion of fruit contaminated by bat saliva or urine is thought to have led to virus spillover into the pigs.
While the Nipah virus wasn’t killing the bats, it was harmful to the pigs, and later to the farmers and butchers handling them, Ellis says. There were nearly 300 human cases and more than 100 deaths, an approximate 40% fatality rate. To stop the outbreak, more than a million pigs were euthanized.
“There are many things we can do to reduce wildlife to human disease transmission,” Ellis says, including the reduction of legal and illegal animal trafficking. Curbing the wild animal trade will reduce the likelihood of emerging zoonotic diseases, she says.
This includes not only wet markets, but practices in the U.S. as well. Ellis points to the Netflix phenomenon “Tiger King”as an example of the pervasiveness of the exotic wild animal trade within American borders.
The underfunding for combatting infectious diseases can harm all of society.
Harsha Thirumurthy, associate director of the Center for Health Incentives and Behavorial Economics
The trade and consumption of wildlife is one cause of outbreaks, Ellis says. “There’s also over-exploitation—taking too many wild animals out of the environment—which changes ecosystem and food dynamics. Some species become too prevalent, others too rare. This can have disease outbreak consequences.”
Ellis notes that emerging infectious diseases are not limited to exotic markets and tropical jungles. “We think of infectious diseases emerging in foreign places, but all you have to do is look in your own backyard to Lyme disease,” Ellis says. Deforestation and habitat fragmentation in the northeastern United States reduced mammal diversity, creating an environment less hospitable to predators and more hospitable to small mammals like the white-footed mouse. More mice mean more meals for infected Ixodid ticks and higher exposure to Lyme disease for both deer and humans.
“We think of this as a foreign problem. But it’s all of us. We’re all doing it,” Ellis says.
McKay is a medical anthropologist. Over the last 15 years, much of her fieldwork has been centered in Mozambique, where she has studied how populations respond to epidemic disease.
“I think that historical and anthropological training can bring a variety of things for global health and medicine,” McKay says, “including thinking about the role of social relationships and social perspectives, how we conduct research around health, and what kinds of social forces shape who gets access to care, and what that care looks like.”
RELATED
Anthropological and historical perspectives also bring the benefits of comparison. While Ebola is transmitted via bodily fluids instead of through close contact droplet transmission like COVID-19, studies of community responses showed how people still had to modify their behaviors in order to maximize survival during the Ebola outbreak, McKay says. This included increased hand washing, limiting everyday forms of physical contact, and changing funeral practices—all seen during the current COVID-19 pandemic as well. Successful responses, McKay says, were able to “recognize the importance of social bonds but also keep people safe.”
“Many communities came up with systems like appointing one person in a household who would take care of people who are sick,” McKay says. “So there’s a lot of similarities [to COVID-19] in terms of thinking how we physically relate to people within a space.”
“One of the things that I have learned from research is the centrality of social relations,” McKay says. “Health is produced through people caring for one another.”
McKay notes that she sees this on the local level in the U.S., in both personal and professional settings. “I think that those unquantifiable aspects of how people are willing to care for one another have tremendous impact on health and well-being,” McKay says. “One of the things social distancing has made visible is that whether or not I take care of my own health has impact on other people.”
Health and poverty
Because health is interdependent, McKay says, “a health care system that is inequitably distributing resources is going to exacerbate future disease.” Her research includes looking at the role of non-governmental organizations (NGOs), which have a vital role in health care funding but don’t necessarily target baseline health needs.
A government health center in Siaya County, Kenya.
“There is this irresolvable debate between people who say that primary care has to be the starting point and people who say that those who live in places without great health care access still have complex needs,” McKay says. She thinks both primary and specialized health care are needed but notes, “one of the things that’s becoming evident with COVID-19 [is that] unless patients who are not feeling well can get seen at the primary level, we can’t serve their specialized needs.”
Funds and programs directed at a single disease can impact health care as a whole, McKay says. “Those kinds of programs can bring really important resources and funding but they can inadvertently weaken broad-based health care.” These “charismatic diseases,” McKay notes, can be a call to arms for donors, but don’t necessarily raise baseline levels of public health.
This baseline is an indicator for how populations respond to health threats. According to Thirumurthy’s “Ending Pandemics” paper, infectious diseases drive global inequality and the effects of pandemics are disproportionately experienced by the poor and marginalized. This is playing out with COVID-19 both within countries (with areas like Detroit being particularly hard-hit) and around the world.
“There is this very strong bidirectional relationship” between health and poverty, Thirumurthy says. “Health is viewed as a byproduct of poverty, when in fact what might be keeping individuals from escaping poverty is their poor health.”
So far, countries that have experienced high numbers of cases during the COVID-19 pandemic include wealthier countries in Europe and Asia. When the case numbers grow in developing countries, the effects are going to be felt more keenly, Thirumurthy says.
In these regions, most people are employed through the informal sector, which includes agriculture as well as buying and selling of goods and services. In this economic structure, “the impact is very broad,” Thirumurthy says. “There is this really strong tension between the policy measures that countries have to take to control the spread of coronavirus and the ability of many people living at the margin to maintain basic living standards.”
Basic health care, not a magic bullet, can often be the difference between life and death.
David Barnes, associate professor of history and sociology of science in the School of Arts & Sciences
If a broad segment of the population can’t afford to stop working, they’re either continuing to go out and put themselves and their communities at risk or they’re falling deeper into poverty, further endangering their own health, he says.
Thirumurthy and a team of researchers from The Center for Health Incentives and Behavioral Economics prepared a set of guidelines and recommendations for policymakers in low-income countries as they consider coronavirus response strategies. “The underfunding for combatting infectious diseases can harm all of society,” Thirumurthy says, and this is “much more stark in many parts of the world.”
Supportive care as cure
One way to treat disease on a fundamental level is through supportive care, says David Barnes of the School of Arts & Sciences. Barnes studies epidemiology, public health, and the history of infectious disease. One of the motifs he has noticed is the capacity of baseline health to ward off illness and the role of supportive care in treatment.
His research has taken him to the Lazaretto, a historic Philadelphia quarantine hospital where a large number of patients were treated for yellow fever, which is transmitted through infected mosquitos, and typhus, a bacterial disease spread by fleas, lice, and chiggers. “The Lazaretto,” Barnes says, “received a lot of patients who were desperately ill and a surprising number of them that were discharged and ‘cured.’” The records show that 75% of patients with yellow fever were listed as cured along with a full 95% of typhus patients, Barnes says.
(Pre-pandemic image) Harsha Thirumurthy and colleagues from Impact Research and Development Organization in Kenya completed an NIH-funded HIV prevention research project before bringing their work online.
“I thought that was hilarious because there’s no cure for yellow fever,” Barnes says. “Typhus is treatable with broad-spectrum antibiotics today, but that certainly wasn’t available then.” His research showed that patients received none of the bloodletting or depletion systems still common during the 18th century, but instead received basic nursing care: clean bedding, clean clothes, meals, fluids, and rest.
This supportive treatment resulted in healthier patients. Barnes noted this during the Ebola epidemic as well. While the average fatality rate was 50%, patients correctly diagnosed and treated in the U.S. or Europe often survived.
“Ebola was, of course, incurable,” Barnes says. “Not a single one of them got a miracle drug or experimental treatment. They got IV rehydration and basic nursing care. This could be the explanation for why the Lazaretto patients survived. Basic health care, not a magic bullet, can often be the difference between life and death.”
While there is now a vaccine for the Ebola virus, Barnes believes this evidence shows that supportive medicine can be crucial in saving lives. “Palliative care works,” he says. “Palliative care heals.”
It is also harder to fund. “Now that we have a vaccine [for the Ebola virus], it doesn’t seem to be a priority to go back to sub-Saharan Africa that has underfunded medical infrastructure. It doesn’t touch that part of our brain,” Barnes says.
Going forward, it really does behoove us to try to work harder to eliminate those disparities before they become exploited by another health problem.
Ezekiel J. Emanuel, vice provost for Global Initiatives, chair of the Department of Medical Ethics and Health Policy
“I worry that we’re going to do the same thing with this disease,” Barnes says of COVID-19. “We’re going to obsess about disease-specific prevention and treatment. We’re going to ignore, relatively speaking, non-disease specific prevention and treatment.” More beds and basic machines are not nearly as satisfying as a vaccine, Barnes says, but could save more lives.
Death rates from infectious diseases have declined steadily because of improving standards of living, Barnes says. “I worry when I see politicians saying, ‘if we can accelerate research into a vaccine and flatten the curve…’”
There’s a limit to how fast a vaccine can be produced, tested, and distributed, Barnes says. “I worry that it will only be available when this epidemic has run its course… I worry that the next pandemic that comes around will be a new germ and we will only have our basic immunity to fight it.”
Barnes advocates for investment in basic health infrastructure, including universal health care and public policies that support stronger, healthier bodies. “It’s like preventing fires by clearing dry brush,” he says. “You don’t just prevent fires by buying new fire engines.”
The economics of global public health
In the meantime, novel disease outbreaks are increasing in both number and diversity, Thirumurthy’s research shows, estimating that the impact of a novel influenza would range from $60 to $80 billion. Strategic investment in a coordinated global health response would have a return ratio of between $17-20 for every $1 spent. These figures jump to more than $100 per $1 if the value of lives lost are included, in addition to income. Increasing pandemic-related funding, Thirumurthy says, would bolster the economy.
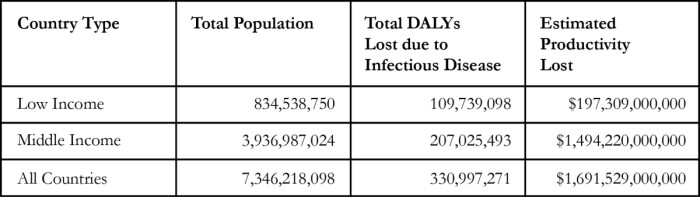
95.7% of disability-adjusted life years lost due to infectious diseases are in low and middle-income countries, even though they account for just 65% of the world’s population, according to "Ending Pandemics," co-authored by Harsha Thirumurthy.
Nevertheless, support for global public health accounts for about 0.2% of the U.S. budget, as health has not been viewed as a good investment, Thirumurthy says. “Historically, economists initially viewed other forms of human capital—education, infrastructure—as generating much higher returns to a country’s economy. Health was not viewed as a priority sector.”
Infectious diseases are responsible for more than 300 million disability-adjusted life years lost, an estimated cost of $1.695 trillion according to "Ending Pandemics," co-authored by Harsha Thirumurthy.
He counters that health is central to the ability of households and communities to economically thrive. “Not only,” Thirumurthy says, is health care spending in low-income countries “a good investment for what it does to improve health, but the U.S. also stands to gain a lot when you consider that infectious diseases can cross borders.”
Thirumurthy sees the ability to prevent the long-term spread of COVID-19 as dependent on the global ability to mount a rapid and aggressive response, yet different countries have differing resources. “Hopefully the U.S. and Europe will be out of the woods and flatten the curve, but our ability to prevent the long-term spread of coronavirus is dependent on low-and middle-income countries’ ability to combat coronavirus,” Thirumurthy says.
He would advise the World Bank to make resources available to low- and mid-income countries. “One of the things that is necessary is for the global community to come together and invest. We are keenly aware of the shortage of equipment if we were to experience a surge in cases in the U.S. It won’t be a surprise that the health systems in low-income countries are even less prepared to handle such surges.”
Justice and health
Preventing future pandemics is ultimately a matter of justice, argues Jennifer Prah Ruger in her recently published book, “Global Health Justice and Governance.” “What is the moral soundness of a set of policies and practices that focuses on politics when what the world needs is scientific guidelines for global health protection?” she asks. Universal health care and the financial means to secure it are vital for global public health, she says.
Prah Ruger is concerned about the influence of geopolitics in global health governance and how it can thwart efforts to fight the pandemic. “Why are we quibbling about how much power and influence a particular country—say China or the United States—has in getting its way, rather than how we can cooperate to stop COVID-19?”
The reformation of global health governance needs to be focused on the common good worldwide, Prah Ruger says. “Legitimate and trustworthy global health institutions that focus on global health equity, regardless of where one lives or what country one represents” are vital, she says. Prah Ruger proposes a Global Health Constitution and a Global Institute of Health and Medicine as alternative governance structures to coordinate independent yet interdependent actors in global health.
Predictions and recommendations
In an April 7 conversation with Perry World House, Zeke Emanuel noted that while the health infrastructure is not robust, sub-Saharan Africa has several advantages over Europe and the U.S., including an age distribution that skews younger, less cross-border traffic, and in some regions, larger rural populations. “Dispersion will slow things down,” he said.
Nevertheless, Emanuel expects to see higher mortality rates (in the range of 1-2% vs. under 1%) due to the lack of hospital beds, supplies, equipment, and staff to provide care. The best hope, he said, is that the spread of COVID-19 will “slow enough that the big hits won’t happen until we have a vaccine.”
Emanuel also advocates for collaboration in public health. “Existing disparities in health status are being exacerbated by this problem,” he said. “Going forward, it really does behoove us to try to work harder to eliminate those disparities before they become exploited by another health problem.”
Barnes, McKay, Prah Ruger, and Ellis all emphasize the interdependence of global health. “We’re all healthier if we’re all healthier,” McKay says. “Our health is always dependent on other people.”
To prevent pandemics, Ellis says, “take care of nature. Stop cutting down tropical rainforests. Consider what wildlife we eat and trade as pets.”
“One thing we could do to reduce pandemic threats is increase people’s food security,” Ellis says, noting that bush meat consumption is often driven by hunger. “Alleviating poverty and food security would go a long way towards reducing pandemics.”
Barnes points to the way these disparities lower the bar for public health and pushes to raise the baseline standard of living. “If we want to fight successfully against coronavirus—and if we want a healthier society—we have to start seeing past germs, and work to strengthen immunity,” Barnes says.
He advocates for a robust investment in supportive care, in addition to the investment in pandemic-related funding that Thirumurthy’s research has shown to be economically vital. “Disease knows no borders,” Thirumurthy says.
“Certainly,” McKay says, “there’s a lesson that we need to take pandemic prevention that much more seriously.”
Novel plant-based approach to a better, cheaper GLP-1 delivery system
Research led by Penn Dental’s Henry Daniell investigates the use of a lettuce-based, plant-encapsulated delivery platform as a new oral delivery of two GLP-1 drugs previously approved by the FDA in injectable form.
No brain, no gain: Neuronal activity enhances benefits of exercise
Research led by Penn neuroscientist J. Nicholas Betley and collaborators finds that hypothalamic neurons are essential for translating physical exertion into endurance, potentially opening the door to exercise-mimicking therapies.
In honor of Valentine's Day, and as a way of fostering community in her Shakespeare in Love course, Becky Friedman took her students to the University Club for lunch one class period. They talked about the movie "Shakespeare in Love," as part of a broader conversation on how Shakespeare's works are adapted.
In Becky Friedman’s English course Shakespeare in Love, undergraduate students analyze language, genre, and adaptation in the Bard’s plays through the lens of love.
Beating the heat: Designing cooling for bodies in motion
Dorit Aviv, director of Weitzman’s Thermal Architecture Lab, studies how humans, technology, and design intersect, paving the way for the development of novel approaches to cooling people efficiently.









{kind=link}
{kind=link}
{kind=link}
{kind=link}