Treatments and vaccines are only useful in the hands of the people who need them, and Penn Medicine is working toward better access and equity for biomedical innovations.
Penn Medicine has a remarkable track record developing therapies that receive FDA approvals, including pioneering whole classes such as cellular and gene therapies and mRNA vaccines. Even so, faculty remain humbled by one basic tenet: Advances mean nothing if patients can’t access them.
“If our goal is to improve human health, we cannot call ourselves successful unless we bring the fruits of our labor to bear as broadly as possible on people suffering from the conditions that interventions are designed to treat,” says Emma Meagher, senior vice dean for clinical and translational research in the Perelman School of Medicine.
Commercialized drug prices are beyond an academic institution’s control, but researchers—including many at Penn—are exploring advances that would make cutting-edge treatments more easily available to everyone who needs them. In the case of CAR T, for example, those working to develop a universal version of the therapy understand they can drive down costs by transforming a time-intensive, personalized treatment that requires a patient to donate their own T cells into one where an existing bank of cells could be used to treat many patients.
Racial and ethnic health disparities also stoke accessibility concerns. Black Americans are less likely than any other group to receive CAR T cell therapy—a trend rooted in gaps in income, education, housing, job security, and proximity to high-quality medical centers. These same social determinants of health have also led to their underrepresentation in CAR T and all kinds of clinical trials; Black patients account for just 5% of clinical trial participants nationwide.
“Black patients’ historically low participation in trials means that, compared to white individuals, they have less access to some of the most advanced new treatments,” says Carmen Guerra, vice chair of diversity and inclusion in the Department of Medicine and associate director of diversity and outreach at the Abramson Cancer Center (ACC).
To better diversify clinical studies in cancer, the ACC recently conducted a five-year community engagement study that reached more than 10,000 individuals through marketing campaigns tailored to minority cultures; wellness forums and events in Black communities; partnerships with Lyft and Ride Health to reduce transportation barriers; and patient education efforts. By the end of the project, the number of Black patients in Penn’s cancer clinical trials had doubled.
Even when drugs are relatively affordable and easy to produce, racial disparities persist—disparities Penn Medicine is striving to overcome. Following the approval of mRNA vaccines against COVID-19, for instance, the health system worked with partners in West and Southwest Philadelphia to bring vaccines directly to their predominantly Black communities in spaces like gyms and public schools, and later moved portable “hyperlocal” clinics between locations like fast-food restaurants and retail parking lots in neighborhoods where many residents remained unvaccinated.
Efforts at Penn to understand gaps in new drug access go as far as examining how and where products end up being prescribed. The next step is figuring out why more people aren’t accessing a drug that could extend or save their lives and how to help close the gap.
“In academics, our incentive mechanism is to publish, to write grants, to see patients, and to teach,” Meagher says. “But if community isn’t an integral, systematic part of our processes, we aren’t doing our jobs to the best of our ability. If you believe what you’re working on is important, you must bring it to all the people it will benefit.”
Penn engineers and collaborators have developed a transparent, micro-engineered device that houses a living, vascularized model of human lung cancer—a “tumor on a chip”—and show that the diabetes drug vildagliptin helps more CAR T cells break through the tumor’s defenses and attack it effectively.
Tumor-on-a-chip offers insight into cancer-fighting cells in immunotherapy
Penn engineers and collaborators have built a living tumor on a chip to expose how cancers block immune attacks, and how one existing drug could make immunotherapy like CAR T more effective against solid tumors.
Professor of city and regional planning Erick Guerra recently published a book exploring the economic and societal impacts of American highways. He explains some of the pitfalls associated with an ever-expansive highway system, arguing that spending more on highways might not be the solution to the country’s transportation issues.
Penn urban planner Erick Guerra’s new book, “Overbuilt,” argues that additional spending on building more highways might not be the solution to the country’s transportation issues. In a Q&A, Guerra shares his insights.
Xin Sun prepares samples collected from the Eastern Tropical North Pacific aboard a research vessel. By adding stable isotope tracers to these vials, Sun and her team can track how different microbial groups convert nitrogen compounds into nitrous oxide, revealing how subtle shifts in oxygen and organic matter change the ocean’s chemistry.
Can tiny ocean organisms offer the key to better climate modeling?
In the shadowy layers of the Pacific, microbes decide how much nitrous oxide—a potent greenhouse gas—rises skyward. New research from Penn’s Xin Sun offers an improved understanding of microbial ecology and geochemistry—key to forecasting global emissions in response to natural and man-made climate change.
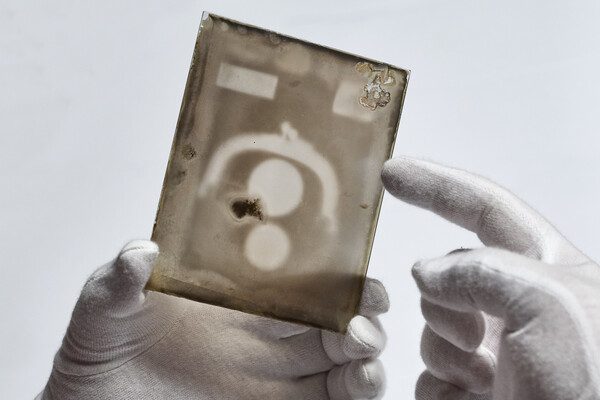
Two X-ray plates from Arthur Goodspeed, believed to have created the world’s first X-ray image, were donated by his family to Penn’s University Archives.




{kind=link}