A groundbreaking genetic study seeks to transform the prevention and treatment of glaucoma while reversing historical racial disparities in who suffers from the disease, and who benefits from such research.
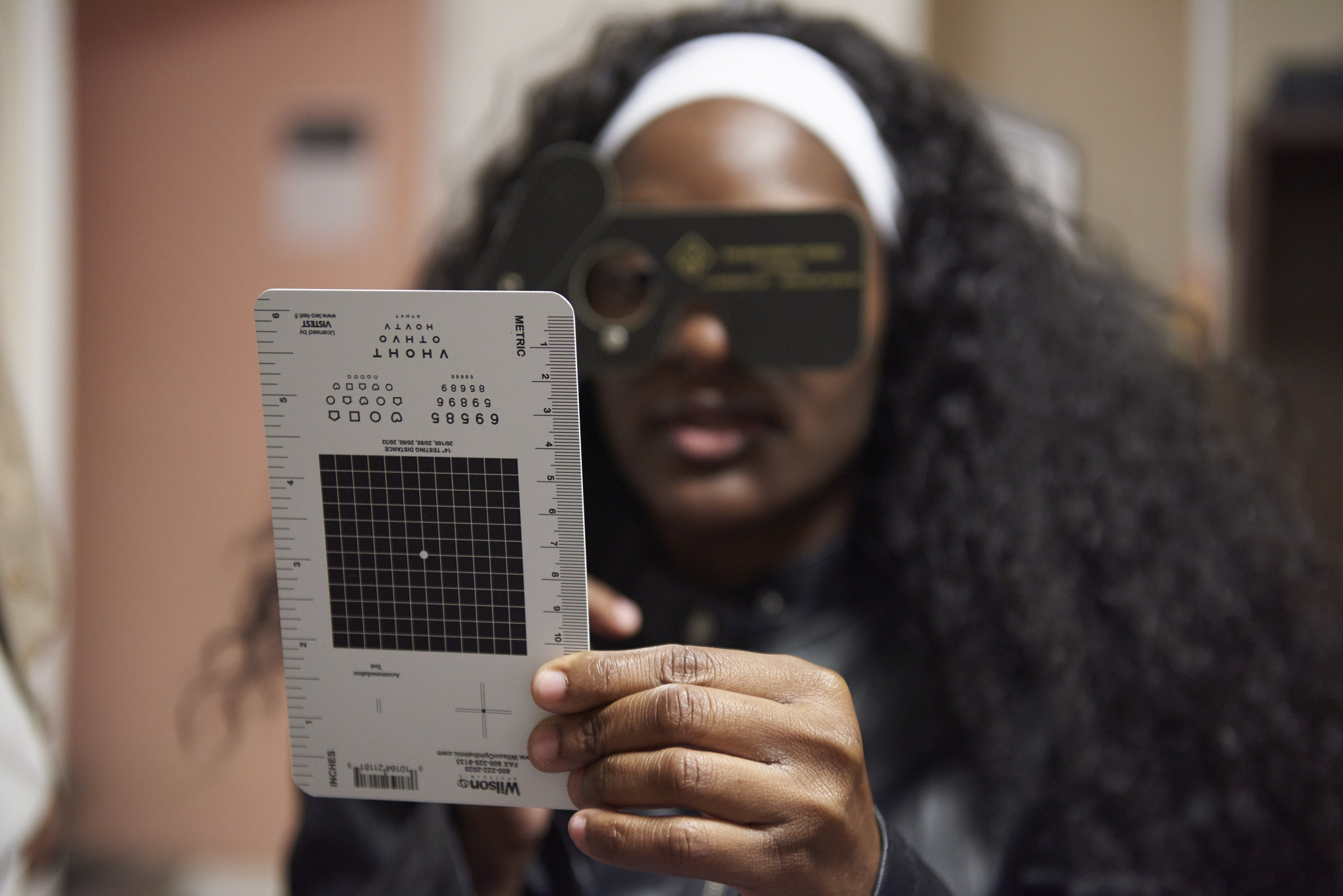
With a mobile glaucoma screening bus funded by the Primary Open-Angle African American Glaucoma Genetics (POAAGG) study, Scheie Eye Institute physicians and staff conduct free community screenings at community centers, churches, and health fairs across the city, including this North Philadelphia health fair.
The human eye is a wonder. It is often said to be the second most complex organ in the human body, outranked only by the brain, and is responsible for transporting visual cues that help process everything from images and memories to thoughts and speech. Doctors who study the eye often find themselves tracing winding pathways among the more than 1 million tangled nerve fibers that connect each eye to the brain. Its inscrutability led some early physicians to theorize that the pupil was nothing more than an indecipherable black hole.
Glaucoma, one of the most debilitating diseases of the eye, is a mystery unto itself. For the more than 3 million Americans living with the disease, there are often no warning signs, no nagging flashes of light or foggy gray circles obstructing views. There is no pain. Then slowly, over time, sharp images may reduce to narrow vignettes; the central portrait is still somewhat recognizable, the outer edges, an infinite blur. Simple tasks like reading and writing may require magnifying devices. For some, daily rituals like driving and shopping become impossible to complete without assistance, until one day, everything fades to black.
With open-angle glaucoma, the form affecting roughly 90 percent of glaucoma patients, everything seems fine until it isn’t; once vision loss occurs, it can’t be reversed.
There is no cure. Its cause is unclear. And though efforts to understand such vision losses date back as far as Hippocrates, much about glaucoma remains a mystery to both the patients living with it and the doctors and scientists who are working to treat it.
The treatment of glaucoma has remained remarkably similar over time, but today, a major study is also using modern genetic science to advance understanding of the disease—and upending a longstanding disparity in who benefits from such research.
It wasn’t until the mid-1800s that the invention of a small handheld device made of half-silvered mirrors and glass plates revolutionized the study of the human eye. The ophthalmoscope enabled early physicians to examine previously obscure parts of the eye and detect dysfunction in central and peripheral vision. In 1862, a Dutch ophthalmologist using the ophthalmoscope identified a connection between high intraocular pressure and blindness, making it possible to diagnose the onset of the condition now known as open-angle glaucoma.
More than a century and a half later, while the ophthalmoscope has seen many functional upgrades, the treatment of glaucoma has remained remarkably similar over time, with the main treatment options focused on lowering the pressure in the eye. But, today, a major study is also using modern genetic science to advance understanding of the disease—and upending a longstanding disparity in who benefits from such research at the same time.
Following the path of genetics
For nearly two years, Kevin Richardson, 52, had been experiencing blurry vision and trouble focusing when reading. Knowing that glaucoma runs in his family—his grandmother had been diagnosed with the disease during her final year of life—in late 2017, Richardson came in to the Scheie Eye Institute at Penn Medicine for an eye exam.
“It’s kind of scary,” he says with a pause, seriously pondering the gravity of his potential risk. “No one wants to lose their eyesight. So I knew I had to come in and find out what it meant for me.”
During his visit, Richardson was approached about enrolling in a study. He would have to provide a DNA sample, and his genes would be sequenced to identify possible genetic variants that might contribute to the risk of glaucoma. He gladly agreed to participate.
“I said yes because I was curious to know more about glaucoma,” he says. “And they all seemed like they really cared about helping me. They went into detail, explaining how everything would work.”
Joan O’Brien, director of the Scheie Eye Institute, is principal investigator of the POAAGG study. She has a track record of bringing precision medicine approaches to ophthalmology.
The study Richardson is taking part in is a large and ambitious one, known as the Primary Open-Angle African American Glaucoma Genetics (POAAGG) study. It launched in 2014, when Joan O’Brien, the director of the Scheie Eye Institute and chairman of ophthalmology at Penn Medicine, received an $11.2 million grant from the National Institutes of Health (NIH). Led by O’Brien as principal investigator with co-investigators Privthi S. Sankar, Eydie Miller, Victoria Addis, and Qi Cui, the five-year study seeks to identify genetic risk factors that contribute to a disproportionately high incidence of primary open-angle glaucoma (POAG) among African Americans.
The study aims to not only correct a health disparity, but to keep Penn Medicine and Penn patients like Richardson at the forefront of transformations in ophthalmology that are bringing precision to the understanding and treatment of eye disease.
Precision medicine—a fairly novel approach that looks to genetic information to create specialized treatments for an individual’s clinical care—is one of the biggest buzzwords of the last decade in medical research. It has worked wonders in the study of cancer, transforming understanding of the disease and enabling doctors to use information about the mechanism of disease to determine which treatment will work best for each patient.
When I came here, I wanted to establish a good infrastructure to take research from bench to bedside to benefit patients.
Joan O’Brien, the director of the Scheie Eye Institute and chairman of ophthalmology at Penn Medicine
O’Brien, the leader of the POAAGG study, has a track record of bringing precision approaches to ophthalmology, having studied the genetics of ocular cancers such as ocular melanoma and retinoblastoma since the late 1980s following her days at Dartmouth Medical School. Her training included an internship in internal medicine (Beth Israel Hospital), residency in ophthalmology (Harvard’s Eye and Ear Infirmary), and fellowships in immunology and ophthalmic pathology (Harvard Medical School), in genetics (Weinberg Lab of the Massachusetts Institute of Technology’s Whitehead Institute), and in ocular oncology (University of California, San Francisco—UCSF).
When she later served as a professor, vice chair of ophthalmology and director of the Ocular Oncology Division at UCSF, much of O’Brien’s NIH-funded research focused on identifying unique pathogenic variants in the retinoblastoma gene (RB1) in an effort to establish targeted therapies to treat the disease based on each patient’s underlying genetic risk. This work resulted in new retinoblastoma therapies being offered nationwide to patients. O’Brien also worked with dermatopathologist Boris Bastian to identify GNAQ and GNA11, genetic variants associated with uveal melanoma. This work was published in Nature and New England Journal of Medicine.
When O’Brien moved to Philadelphia in 2010 and became the eighth chairman of ophthalmology at the Perelman School of Medicine, she hoped to make another similar impact through precision medicine.
“When I came here, I wanted to establish a good infrastructure to take research from bench to bedside to benefit patients,” O’Brien says. “So, I wanted to investigate a disease to address an unmet need in Philadelphia.”
It didn’t take long to find. O’Brien and her team noticed a staggering number of particularly young African-American residents, many in their 30s and 40s, who were coming to their practice in West Philadelphia seeking treatment for moderate to severe vision loss.
“It was really frustrating to see someone in the prime of their life be disabled in that way,” recalls Prithvi S. Sankar, a professor of clinical ophthalmology. “It was heartbreaking.”
Overburdened, yet underrepresented
The local cases seemed to mirror national statistics. Glaucoma is the leading cause of irreversible blindness in the world today. As studies show, African Americans are four to five times more likely to have glaucoma than Caucasians. Glaucoma also tends to appear earlier and progress faster in African Americans. Open-angle glaucoma can occur when drainage canals in the eye become clogged over time, leading to increased eye pressure. Because the disease progresses slowly over time, more than half of the individuals living with the disease are unaware that they have it.
A community member at a health fair undergoes a near visual acuity test.
It is unclear why African Americans are more frequently affected with more severe cases of the disease than other ethnic populations or groups. In many cases, racial and ethnic disparities in health can be attributed to social causes, including the persistent impacts of inequality in income, housing, education, access to health care, and more. When it comes to primary open-angle glaucoma, strong correlations exist between the disease and family history. O’Brien notes that an individual’s risk of developing glaucoma increases up to tenfold when a parent or sibling has the disease. This pattern holds true in high-risk populations of African descent, yet the genetics of the disease in general are poorly understood. O’Brien therefore believes that key answers that could offer benefits to African-American patients who are disproportionately burdened with glaucoma may lie in novel genetic research.
3% of samples
A 2016 analysis published in Nature by researchers at the University of Washington found that people of European ancestry continue to dominate this type of research. Their analysis comprised more than 2,500 studies with 35 million genetic samples. A mere 3 percent of those samples came from people with African ancestry. Data source: Popejoy & Fullerton, Nature, October 2016.
Now, with the POAAGG study, the researchers aim to enroll a large study population, especially for a study focused on a minority group: 7,765 African American patients, including 3,000 with primary open-angle glaucoma and 4,765 controls.
O’Brien admits it has been an ambitious undertaking, one with many potential barriers and challenges.
The study is unusual for more than just its size. Historically, genome-wide association studies (GWAS) of this kind have failed to include populations of African descent or other minority groups in the North American and European research centers where many of these studies have been conducted to date. A 2016 study published in Nature found that only 3 percent of GWAS participants were of African ancestry. GWA studies serve as the primary tool for identifying genetic variants in individuals to see which, if any, variants are associated with disease traits. People whose ancestry did not go through a genetic bottleneck in Europe may have the same genetic variants with a different frequency than in European-descended populations, or a broader range of variants in some cases—so when GWA studies focus so narrowly, the understanding of the genetic basis of disease can be incomplete. And because they’ve been historically left out of these studies, populations, such as African Americans, whose ancestry does not primarily trace back through Europe, are less likely to benefit from precision medicine.
Eydie Miller, a co-investigator of the POAAGG study, said she’s proud to be a part of a study that focuses exclusively on African Americans, who have historically been neglected in genetic research.
Eydie Miller argues that part of the reason why African Americans have been underrepresented in GWA studies in the past is investigator bias; researchers may have thought African Americans would not participate and opted not to seek or include them. Miller, a professor of clinical ophthalmology and director of the Glaucoma Service at the Scheie Eye Institute, wasn’t shy about stating her belief that it is “inherently unfair to exclude from GWA studies the population that has the most disability from this disease.” Miller, however, says she’s proud to be a part of a study that focuses exclusively on this historically neglected group.
There are other reasons, too, that have made the researchers’ goal of recruiting more than 7,500 African Americans a formidable pursuit.
The underrepresentation of African Americans in GWA studies may also be attributed to the community’s deep-seated distrust of medicine. O’Brien points to the Tuskegee Experiment and the controversy surrounding HeLa cells as prominent instances where African Americans have been treated unfairly by members of the medical community. This history has led to population-wide hesitation toward participating in medical studies.
Miller says some of the patients she attempted to enroll expressed concerns about participating in this and other studies, considering the history of exploitation as a source of medical knowledge that benefits only white patients. “Some were definitely concerned about the history of research studies with people of African descent and whether there is equity and fairness in terms of diagnosis and management of data dating back to the Tuskegee experiment,” she says.
Building new roads to recruitment
In the early stages of recruitment for the study, O’Brien’s team found success in reaching out to willing patients like Kevin Richardson. The hope was that the grassroots, word-of-mouth approach to outreach would render results.
Sankar admits that, early on, he worried that they might not meet their enrollment goals.
“I think there was this sense within the African American community that they didn’t want to be used as guinea pigs, considering all of the things that have happened in the past,” he says.
To address patients’ concerns of this nature, Miller says, “we go the extra mile in letting them know that their privacy is being respected,” describing details of how data is de-identified to protect participants from insurance discrimination based on genetic risk, and emphasizing the integrity of the process.
In the first year, the researchers were able to recruit a cohort of more than 2,500 participants, the largest African-American primary open-angle glaucoma population recruited at a single institution. To date, more than 9,500 participants have enrolled in the study—in excess of the targeted 7,765 participants, accounting for a number of individuals who had suspected but unconfirmed glaucoma at the time of enrollment. Recruitment is ongoing.
The team has done what Joan O’Brien calls “inreach,” or reaching into the community to connect with groups in forums and settings that they typically would not have access to.
Getting to this point has entailed a broad-based, large-scale outreach strategy. O’Brien’s team began by tapping their closest resources for support, partnering with several local ophthalmologists who volunteered to open their clinics to the study, giving access to a broader pool of patients. An additional 1,600 patients were recruited from the Penn Medicine Biobank, a collection of DNA samples from more than 40,000 Penn patients who have consented to have their DNA used in research studies across the University.
The team also worked to ensure that the study was minimally invasive. In the past, large genetic studies have avoided obtaining DNA samples from saliva because blood samples were considered to be more reliable. But a 2016 analysis published by members of O’Brien’s research team proved that saliva collection is an equally viable alternative to blood collection.
Two years into the study, the researchers replaced blood sample collection with saliva sample collection, a change that Sankar says served as a major benefit to enrollment. Knowledge gained from this change in collection method might also help future genetic studies to be more successful in enrolling patients who might otherwise be hesitant to have their blood drawn to participate.
“People don’t like getting blood drawn,” he explains. “So, being able to have them spit into a tube instead, that was a huge advantage from our standpoint and it bolstered our recruitment significantly.”
The team then began what O’Brien likes to refer to as “inreach” or reaching into the community to connect with groups in forums and settings that they typically would not have access to.
Their efforts led to the creation of a screening clinic at Scheie and a mobile glaucoma screening bus. Both were used to conduct free glaucoma screenings at community centers, health centers, retirement communities, and churches throughout the city, enrolling eligible volunteers in the study along the way.
I’m African American, so when I talk to patients, I put a personal emphasis on it. I let them know that I understand what they’re going through because [glaucoma] runs in my family, too.
Eydie Miller, a professor of clinical ophthalmology and director of the Glaucoma Service at the Scheie Eye Institute
In February 2018, the team began partnering with WURD, an African-American owned and operated talk radio station in Philadelphia, to launch a new multimedia awareness campaign. Radio commercials, digital ads, and flyers offer a phone number for people diagnosed with glaucoma to sign up for the study. Eligible callers are scheduled for appointments at the Scheie Eye Institute, which include free exams and second opinions from glaucoma specialists. “We are hoping this initiative will not only help with study recruitment, but also in developing stronger relationships with the Philadelphia community and raising awareness about glaucoma,” says Ava Kikut, who manages the campaign.
Researchers’ efforts to make a personal connection with the people in the communities they serve have been key to recruitment from the beginning, Miller says. The work hits close to home for her; her mother and several relatives from both sides of her family were diagnosed with glaucoma.
“I’m African American, so when I talk to patients, I put a personal emphasis on it. I let them know that I understand what they’re going through because it runs in my family, too. I try to help them understand that better glaucoma management lies in being able to have a better understanding of the genetic basis of the disease,” she says. “And when I explain to them the good that this will do for their families in the future, they are actually much more open to the idea; they see the bigger picture; they know they’re not being experimented on.”
The researchers emphasized to patients that because the genetic study is seeking a basic understanding of the disease, they may not see an immediate impact in new treatments for themselves—but many patients were pleased to be a part of research that would benefit future patients.
“Anything that might be hereditary is important for people to know,” says Janet L. Williams-Brown, 75, a long-term patient of Scheie and POAAGG study participant whose mother was diagnosed with glaucoma, putting Williams-Brown at a higher risk for having the disease. “I think participating is a good way to pay it forward. I have eight sisters, five brothers, and 32 nieces and nephews; I want them to benefit from this research.”
An expanding spectrum of glaucoma
As O’Brien’s team approaches the final year under the NIH grant, Lab Director and Research Project Manager at the Scheie Eye Institute Harini Gudiseva finds herself at the helm of a massive undertaking. The researchers have begun a comprehensive analysis of data collected over the past four years. Another approach to genetic analysis, whole exome sequencing, is planned for the entire cohort in the coming months.
The hope is that the collected data will confirm their original hypotheses: that genetic variants influence the risk of POAG and the traits related to that risk, such as intraocular pressure and corneal and retinal nerve fiber layer thickness; and that demographic and ocular risk factors, and medical co-morbidities also contribute to the increased risk of POAG in African Americans.
Two years into the study, the team initiated a GWAS to identify the most frequent genetic variants among the first 5,500 enrolled patients. The GWAS enables the researchers to identify variants with a significant association with open-angle glaucoma, as well as variants associated with variables such as intraocular pressure or retinal nerve fiber layer thickness along with other specific glaucoma traits.
In addition, recent studies have indicated possible links between glaucoma and dysfunction in the mitochondria, the energy-generating organelles inside cells that carry distinct DNA that is passed directly from mother to child, unlike the DNA in the cell’s nucleus that mixes genes from both parents. To investigate these potential hereditary links, O’Brien’s team is also using the collected data to study variants in mitochondrial DNA (mtDNA).
O’Brien’s team has now begun the meticulous work of dividing their study participants according to their mtDNA inheritance groupings, called haplogroups, that reflect known maternal lineages. This process will help determine which risk factors are most likely to be found among specific haplogroups, and will ultimately, O’Brien hopes, become one portion of a risk model for POAG in African Americans.
“Once we identify a participant’s haplogroup, we can see—depending upon which haplogroup they’re in—the level of risk they might be facing,” O’Brien explains.
I think participating is a good way to pay it forward. I have eight sisters, five brothers, and 32 nieces and nephews; I want them to benefit from this research.
Janet L. Williams-Brown, 75, a long-term patient of Scheie and POAAGG study participant whose mother was diagnosed with glaucoma
The researchers have produced several publications and have more in preparation that will elucidate the study’s final results in the coming months. In the meantime, O’Brien says, the group may have already made significant progress in identifying variants that may be linked with a higher risk of developing more severe cases of glaucoma.
“We’re still in the process of confirming this, but there appears to be a variant that’s associated with more rapid progression, younger age, and lower pressures,” she says.
Further, the team’s early findings seem to confirm their hypotheses that glaucoma, much like cancer, is not one, but many diseases with various underlying causes and genetic differences. If this is proven to be true, the researchers hope to create named subcategories to identify the various types of glaucoma they encounter. This could enable them to develop precision, targeted treatments for each form of disease.
“Right now, if we look into an optic nerve and see any kind of atrophy, we’re going to call it glaucoma. But if we were neurologists, and we found an abnormality in the brain, we’d do a scan and depending on what we found we might call it frontotemporal dementia or Alzheimer’s or some other neurological disorder,” she explains. “Our early findings indicate that we have to begin to look at glaucoma in the same way. Atrophy of the optic nerve in glaucoma will sometimes coincide with more generalized atrophy seen in dementia. This likely represents a different clinical subtype of glaucoma which demonstrates different genetic markers.”
Spurring future discovery
The POAAGG study—just on the basis of the richness and scale of the data it has collected to date—is likely to spur many future studies of glaucoma as well as fuel collaboration across disciplines to create new treatments for the disease. This, Miller says, is the ultimate goal of the study.
“We’re starting that work by looking at genetics and we’re doing the standard treatment in our office but there are lots of pharmacologists, people who design devices and a whole cadre of people that are necessary to treat any medical disease,” Miller says. “So we want to open up the door for all these other investigators to try to find a better way to prevent blindness.”
Using the POAAGG study data, researchers will be able to explore an array of topics related to disease progression, family history, and risk factors for blindness. Perhaps most importantly, O’Brien argues, the study represents a significant step in closing the gap of underrepresentation of non-European populations in important genetic studies.
In any study, there is of course the possibility that the researchers will be unsuccessful in proving their hypotheses; the POAAGG study is no exception. After a moment of pause, O’Brien acknowledged her ambivalence about the potential outcomes.
“I think this department has an amazing faculty who really want to help their patients in every way. This study is just one example of that,” she says. “If we don’t find really significant variants, I think it would be unfortunate. On the other hand, we’ll have gathered all of this very useful genetic information. So, hopefully some young scientist can use that information to do some groundbreaking work on other diseases that affect this population in the future. Let’s reverse this negative history in science and let’s make this a city where the most overaffected population becomes the most studied population.”
This story was originally published in Penn Medicine magazine.
Homepage photo: Glaucoma, one of the most debilitating diseases of the eye, is a mystery unto itself. For the more than 3 million Americans living with the disease, there are often no warning signs, no nagging flashes of light or foggy gray circles obstructing views.
In Senegal, the ambitious Dakar Greenbelt project seeks to create an extensive network of ecological infrastructure in and around the city to sustainably address environmental concerns and enhance urban life. With support from David Gouverneur and Ellen Neises, Ph.D. candidate Rob Levinthal in the Weitzman School of Design led two courses that included a field trip to Dakar, that culminated in students presenting their visions for parts of the Greenbelt.
From a desert to an oasis: Penn engages in ambitious greening effort in the Sahel
Students from the Weitzman School of Design journeyed to Senegal to help with a massive ecological and infrastructural greening effort as part of their coursework. The Dakar Greenbelt aims to combat desertification and promote sustainable urban growth.
As part of an undergraduate course, Penn faculty and students curated an Arthur Ross Gallery exhibition of works from the Neumann family’s extensive collection of modern and contemporary art.
The University’s nexus for technology transfer supports researchers in their innovative efforts, from CAR T to mRNA advancements that have dramatically reshaped the world.