Comparing urban and rural excess mortality during COVID-19
The first-ever county-level study of excess mortality in the United States shows monthly excess deaths spread from large cities to rural counties in the second year of the pandemic.
The World Health Organization’s latest estimates for COVID-19 deaths worldwide exceeds 3.3 million, yet excess mortality and how the pandemic spread among populations is still being assessed.
In the second year of the COVID-19 pandemic, relative excess mortality increased in rural counties in the U.S. while decreasing in metropolitan ones, according to a new study led by the University of Pennsylvania and Boston University. Published in Science Advances, it’s the first-ever study showing monthly excess deaths at the county level for the first two years of the pandemic.
Researchers say estimates could inform public health workers and residents of the true impact of the pandemic and could increase vaccine uptake.
“Detailed information on the impact of the pandemic can help policymakers make informed choices regarding the appropriate measures to help communities recover from the negative impacts of COVID-19,” says lead author Eugenio Paglino, a doctoral student in the School of Arts & Sciences and the Population Studies Center at Penn. He says he hopes the information “will bring more research into the local determinants of the excess level of mortality, which is very difficult to do if you only have state-level data.”
For example, he says researchers could correlate county-level estimates with an area’s number of hospitals, mitigation measures, economic activity, and distribution of racial and ethnic groups.
Using a model with data from 2015 to 2019, they estimated that 1,179,024 excess deaths occurred in the U.S. between March 2020 and February 2022, meaning that’s how many more people died than would be expected under non-pandemic conditions.
Excess deaths didn’t substantially decrease during the second year: The study identified 634,830 estimated excess deaths in the first year and 544,194 in the second.
Excess mortality includes deaths from COVID-19 but also from indirect factors such as “hospital avoidance due to fear of COVID-19 infection, increases in drug overdoses, and economic hardship leading to housing and food insecurity,” the study states. Excess deaths substantially moved from large metropolitan to nonmetropolitan areas between the first and second year.
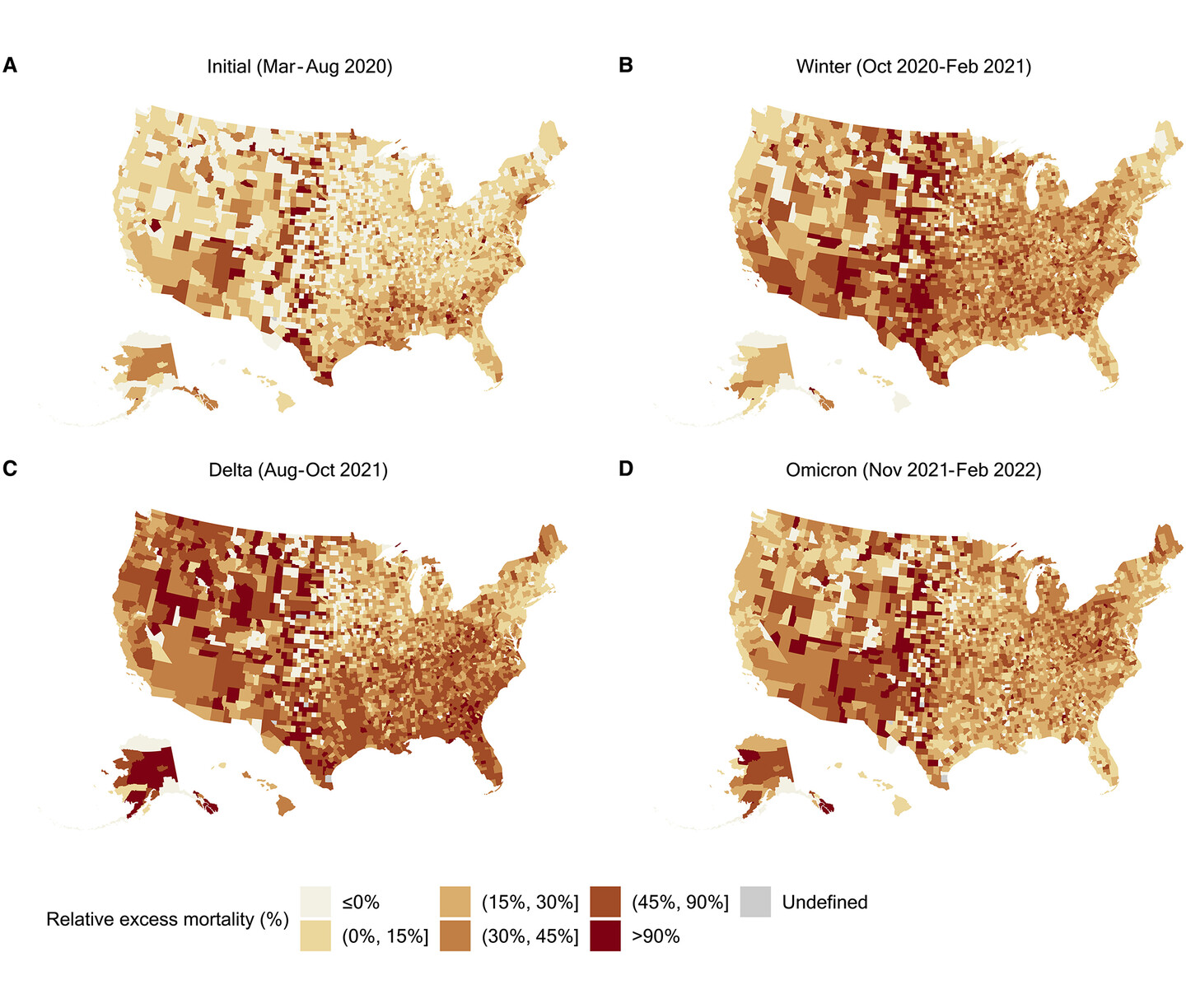
Relative excess mortality—meaning the ratio of excess deaths to expected deaths—across U.S. counties during four mortality peaks in the first two years of the pandemic. Each map refers to a period of particularly high excess mortality.
(Image: Eugenio Paglino and Zhenwei Zhou)
“I think when I came into the study, I thought the pattern followed by large metros, like New York, would have been replicated similarly in other parts of the country,” Paglino says. “Instead, we see even the opposite pattern.”
The study found that among large metropolitan areas, the decrease in excess mortality was most pronounced in the mid-Atlantic, New England, and Pacific areas, whereas the increase in non-metropolitan areas was largest in the Pacific, New England, and mountain regions.
The researchers found that excess mortality became more concentrated in the South and West during the peak of the COVID-19 delta variant, whereas it was less geographically consistent in the omicron variant spike. By February 2022, the largest relative excess mortality was recorded in the nonmetropolitan South.
“The emergence of a rural disadvantage reflects a combination of social, structural, and policy factors, including a lack of state policies designed to protect communities at greatest risk of COVID-19 death, state disinvestment in rural health care and social programs, and vaccine hesitancy fueled by a toxic mix of partisanship and misinformation,” says corresponding author Andrew Stokes, who received his master’s degree and doctorate from Penn and is now an assistant professor at Boston University.
“When the pandemic started in large metro areas of the mid-Atlantic the rest of the country didn’t think they would be affected and viewed it as a ‘big-city problem,’” says Irma Elo, a Penn professor of sociology and co-author on the study. “But what our findings really show is that nobody is safe from the pandemic. The spread may take time, but it’s reaching even the smallest towns in every state.”
This comes, Elo says, after decades of health infrastructure being decimated in rural areas as hospitals have closed.
Vaccine availability was another contributing factor to understanding the shift in urban and rural excess mortality, says co-author Katherine Hempstead, of the Robert Wood Johnson Foundation.
“These results highlight the extent to which excess mortality became a rural phenomenon in year two of the pandemic,” says Hempstead, and reveal "the important role played by protective behaviors, or lack thereof, in rural mortality.”
In future work, the researchers say they plan to study county-level differences in excess mortality by race and ethnicity, gender, and educational attainment.
Paglino says the team is also working on another paper comparing excess death estimates to the official number of COVID-19 deaths. They hope to learn if underreporting of COVID-19 deaths increased or decreased during the pandemic, and to understand which geographic areas have larger gaps in death registration.
“Simply relying on having COVID-19 on the death certificate is inadequate to measure the full impact of the pandemic,” Elo says. She cited lack of testing early in the pandemic, inadequate testing resources in rural areas, and other chronic conditions being listed on the death certificates of people who never got tested for COVID-19.
Elo says next steps include looking at county-level characteristics of areas with high excess mortality and studying the pandemic’s impact on racial and ethnic minorities, especially immigrant populations.
Eugenio Paglino is a doctoral student in the Department of Sociology in the School of Arts & Sciences and at the Population Studies Center at the University of Pennsylvania.
Irma Elo is a professor in the Department of Sociology and research associate at the Population Studies Center at Penn.
Andrew Stokes is an assistant professor in the Department of Global Health at the School of Public Health at Boston University.
Katherine Hempstead is a senior policy adviser at the Robert Wood Johnson Foundation.
Other co-authors include Penn’s Samuel Preston; Dielle J. Lundberg, Zhenwei Zhou, Rafeya Raquib, and Jacob Bor of Boston University, and Joe A. Wasserman of RTI International. [SLJ8]
The research was supported by the Robert Wood Johnson Foundation (grant 77521), the National Institute on Aging (R01-AG060115-04 and 01-AG060115-04S1), the W.K. Kellogg Foundation (P-6007864-2022), the Boston University Center for Emerging Infectious Diseases Policy and Research, the Agency for Healthcare Research and Quality (T32HS013853), and the National Institute of Child Health and Human Development (T32HD007242).
Nanoparticle blueprints reveal path to smarter medicines
New research involving Penn Engineering shows detailed variation in lipid nanoparticle size, shape, and internal structure, and finds that such factors correlate with how well they deliver therapeutic cargo to a particular destination.
A generous gift from alumni Glenn and Amanda Fuhrman brings the work of internationally acclaimed artist Jaume Plensa to the University of Pennsylvania. The latest addition to the Penn Art Collection expands Philadelphia's public art.
A massive chunk of ice, a new laser, and new information on sea-level rise
For nearly a decade, Leigh Stearns and collaborators aimed a laser scanner system at Greenland’s Helheim Glacier. Their long-running survey reveals that Helheim’s massive calving events don’t behave the way scientists once thought, reframing how ice loss contributes to sea-level rise.





{kind=link}
{kind=link}